Buonocore Federica, Maharaj Avinaash, Qamar Younus, Koehler Katrin, Suntharalingham Jenifer P, Chan Li F, Ferraz-de-Souza Bruno, Hughes Claire R, Lin Lin, Prasad Rathi, Allgrove Jeremy, Andrews Edward T, Buchanan Charles R, Cheetham Tim D, Crowne Elizabeth C, Davies Justin H, Gregory John W, Hindmarsh Peter C, Hulse Tony, Krone Nils P, Shah Pratik, Shaikh M Guftar, Roberts Catherine, Clayton Peter E, Dattani Mehul T, Thomas N Simon, Huebner Angela, Clark Adrian J, Metherell Louise A, Achermann John C
Genetics and Genomic Medicine Research and Teaching Department, UCL Great Ormond Street Institute of Child Health, University College London, London, UK.
Centre for Endocrinology, William Harvey Research Institute, Queen Mary University of London, London, UK.
J Endocr Soc. 2021 May 11;5(8):bvab086. doi: 10.1210/jendso/bvab086. eCollection 2021 Aug 1.
Although primary adrenal insufficiency (PAI) in children and young people is often due to congenital adrenal hyperplasia (CAH) or autoimmunity, other genetic causes occur. The relative prevalence of these conditions is poorly understood.
We investigated genetic causes of PAI in children and young people over a 25 year period.
Unpublished and published data were reviewed for 155 young people in the United Kingdom who underwent genetic analysis for PAI of unknown etiology in three major research centers between 1993 and 2018. We pre-excluded those with CAH, autoimmune, or metabolic causes. We obtained additional data from NR0B1 (DAX-1) clinical testing centers.
Genetic analysis involved a candidate gene approach (1993 onward) or next generation sequencing (NGS; targeted panels, exomes) (2013-2018).
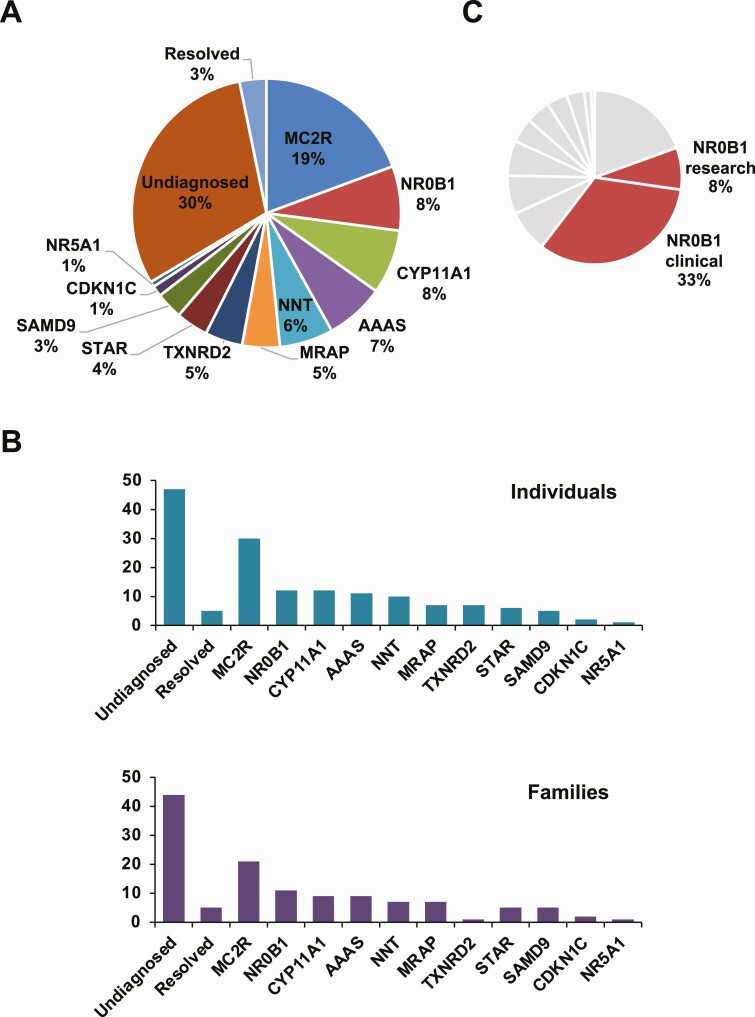
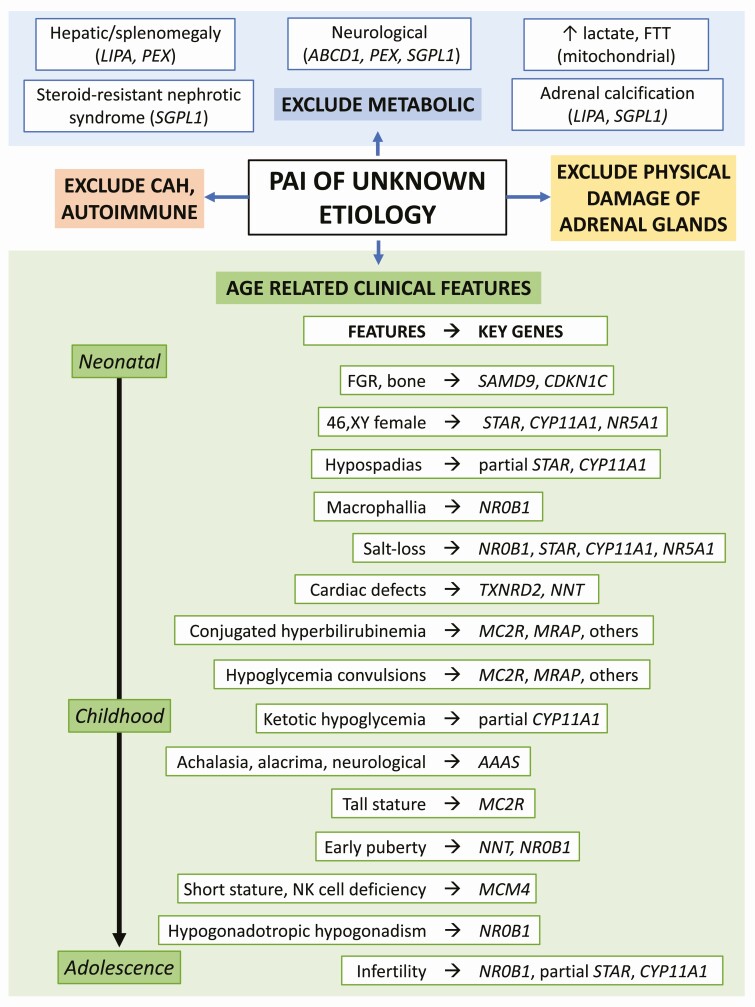
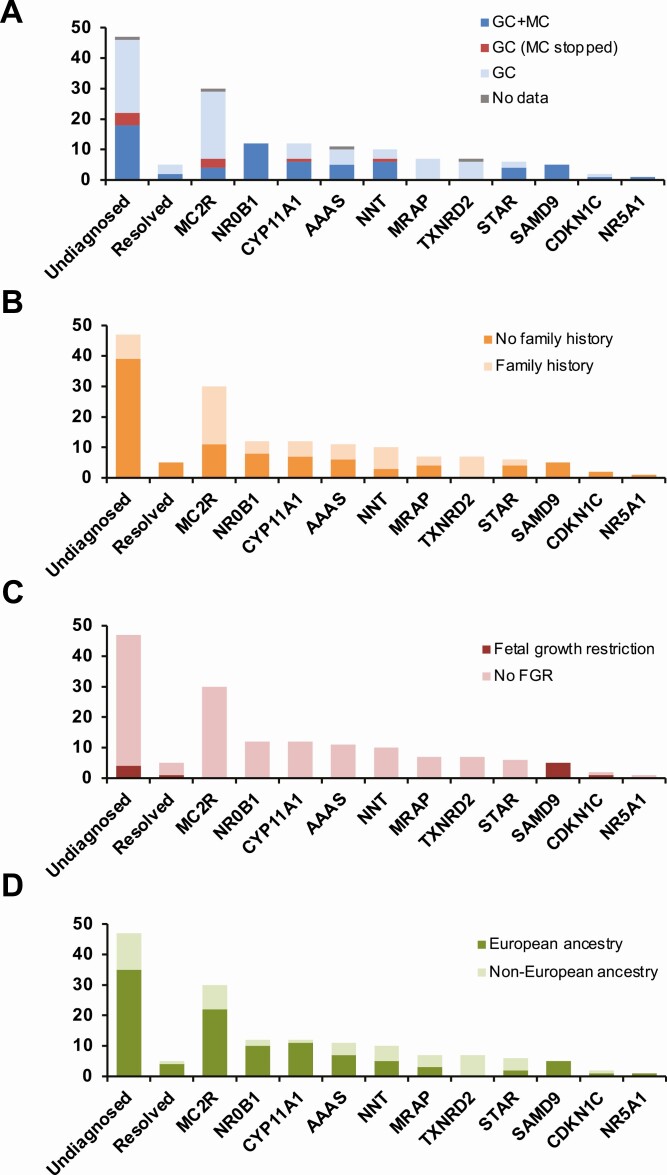
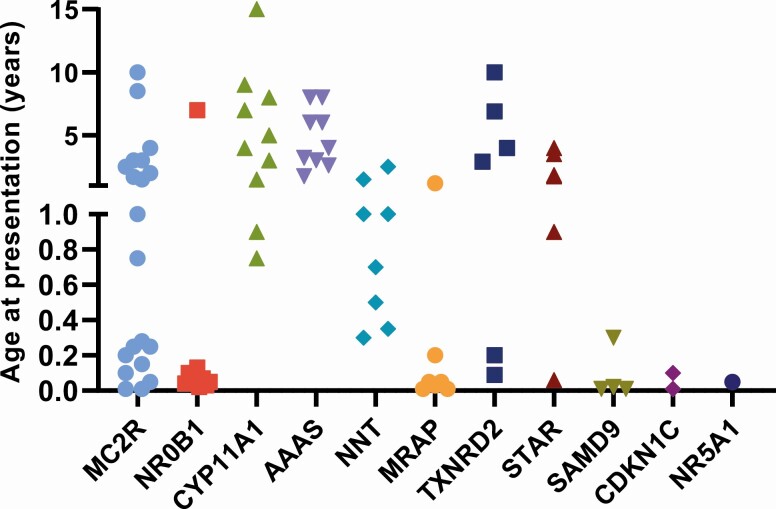
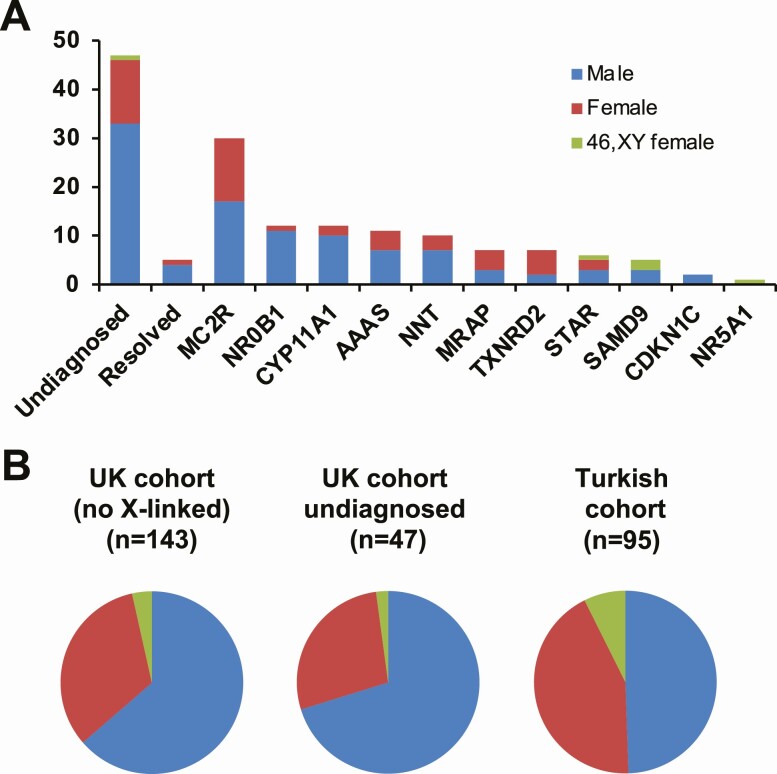
A genetic diagnosis was reached in 103/155 (66.5%) individuals. In 5 children the adrenal insufficiency resolved and no genetic cause was found. Pathogenic variants occurred in 11 genes: (adrenocorticotropin receptor; 30/155, 19.4%), (DAX-1; 7.7%), (7.7%), (7.1%), (6.5%), (4.5%), (4.5%), (3.9%), (3.2%), (1.3%), and /steroidogenic factor-1 (SF-1; 0.6%). Additionally, 51 boys had variants identified through clinical testing. Although age at presentation, treatment, ancestral background, and birthweight can provide diagnostic clues, genetic testing was often needed to define the cause.
PAI in children and young people often has a genetic basis. Establishing the specific etiology can influence management of this lifelong condition. NGS approaches improve the diagnostic yield when many potential candidate genes are involved.
尽管儿童和青少年原发性肾上腺功能不全(PAI)通常由先天性肾上腺增生(CAH)或自身免疫引起,但也存在其他遗传原因。人们对这些疾病的相对患病率了解甚少。
我们调查了25年间儿童和青少年PAI的遗传原因。
设计、地点和参与者:回顾了1993年至2018年间在英国三个主要研究中心对155名病因不明的PAI青少年进行基因分析的未发表和已发表数据。我们预先排除了患有CAH、自身免疫或代谢原因的患者。我们从NR0B1(DAX-1)临床检测中心获得了额外数据。
基因分析采用候选基因方法(1993年起)或下一代测序(NGS;靶向panel、外显子组)(2013 - 2018年)。
103/155(66.5%)个体获得了基因诊断。5名儿童的肾上腺功能不全得到缓解,未发现遗传原因。11个基因中出现了致病变异:促肾上腺皮质激素受体(30/155,19.4%)、DAX-1(7.7%)、(7.7%)、(7.1%)、(6.5%)、(4.5%)、(4.5%)、(3.9%)、(3.2%)、(1.3%)以及/类固醇生成因子-1(SF-1;0.6%)。此外,51名男孩通过临床检测鉴定出了变异。尽管发病年龄、治疗、祖先背景和出生体重可提供诊断线索,但通常仍需要基因检测来确定病因。
儿童和青少年PAI通常具有遗传基础。确定具体病因可影响这种终身疾病的管理。当涉及许多潜在候选基因时,NGS方法可提高诊断率。