General Internal Medicine Department, Hospital Universitario San Juan de Alicante, San Juan de Alicante, Alicante, Spain.
Department of Clinical Medicine, Faculty of Medicine, Miguel Hernández University, Elche, Alicante, Spain.
J Gen Intern Med. 2021 Nov;36(11):3478-3486. doi: 10.1007/s11606-021-07017-8. Epub 2021 Jul 21.
Venous thrombotic events (VTE) are frequent in COVID-19, and elevated plasma D-dimer (pDd) and dyspnea are common in both entities.
To determine the admission pDd cut-off value associated with in-hospital VTE in patients with COVID-19.
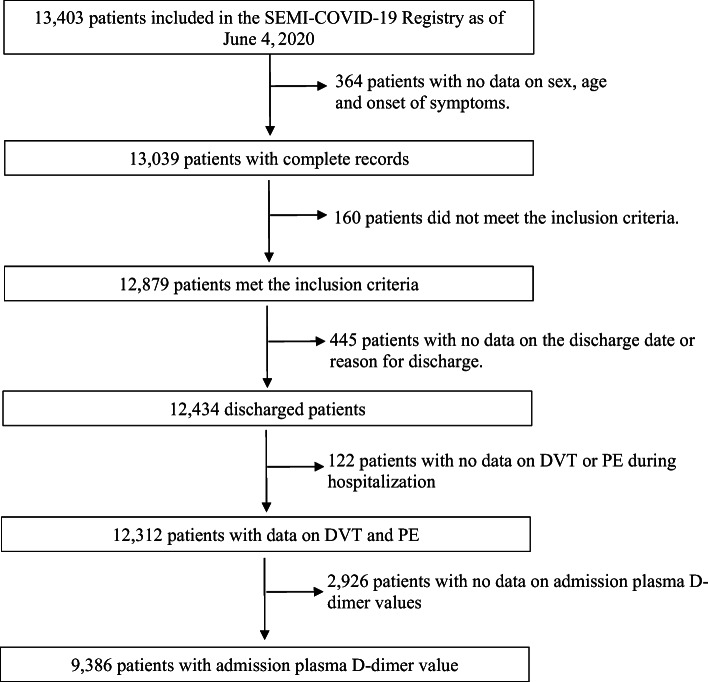
Multicenter, retrospective study analyzing the at-admission pDd cut-off value to predict VTE and anticoagulation intensity along hospitalization due to COVID-19.
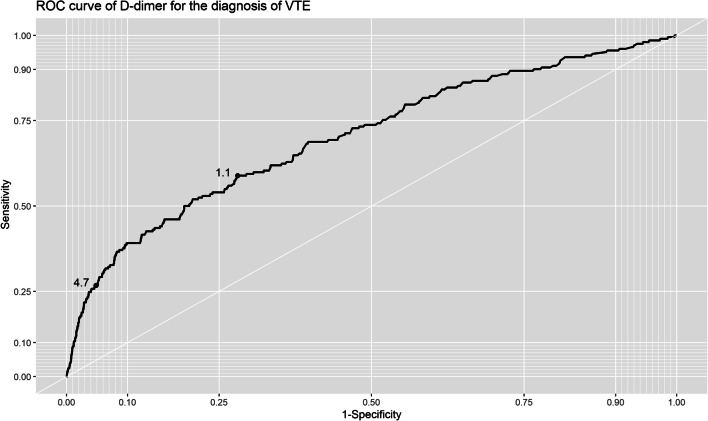
Among 9386 patients, 2.2% had VTE: 1.6% pulmonary embolism (PE), 0.4% deep vein thrombosis (DVT), and 0.2% both. Those with VTE had a higher prevalence of tachypnea (42.9% vs. 31.1%; p = 0.0005), basal O2 saturation <93% (45.4% vs. 33.1%; p = 0.0003), higher at admission pDd (median [IQR]: 1.4 [0.6-5.5] vs. 0.6 [0.4-1.2] μg/ml; p < 0.0001) and platelet count (median [IQR]: 208 [158-289] vs. 189 [148-245] platelets × 10/L; p = 0.0013). A pDd cut-off of 1.1 μg/ml showed specificity 72%, sensitivity 49%, positive predictive value (PPV) 4%, and negative predictive value (NPV) 99% for in-hospital VTE. A cut-off value of 4.7 μg/ml showed specificity of 95%, sensitivity of 27%, PPV of 9%, and NPV of 98%. Overall mortality was proportional to pDd value, with the lowest incidence for each pDd category depending on anticoagulation intensity: 26.3% for those with pDd >1.0 μg/ml treated with prophylactic dose (p < 0.0001), 28.8% for pDd for patients with pDd >2.0 μg/ml treated with intermediate dose (p = 0.0001), and 31.3% for those with pDd >3.0 μg/ml and full anticoagulation (p = 0.0183).
In hospitalized patients with COVID-19, a pDd value greater than 3.0 μg/ml can be considered to screen VTE and to consider full-dose anticoagulation.
COVID-19 患者常发生静脉血栓栓塞事件(VTE),且血浆 D-二聚体(pDd)升高和呼吸困难在这两种情况下均很常见。
确定与 COVID-19 患者住院期间 VTE 相关的入院时 pDd 截断值。
这是一项多中心、回顾性研究,分析了入院时 pDd 截断值,以预测 COVID-19 患者因 VTE 而住院期间的 VTE 和抗凝强度。
在 9386 例患者中,有 2.2%发生了 VTE:1.6%为肺栓塞(PE),0.4%为深静脉血栓形成(DVT),0.2%为两者兼有。有 VTE 的患者呼吸急促的发生率更高(42.9%比 31.1%;p = 0.0005),基础氧饱和度<93%(45.4%比 33.1%;p = 0.0003),入院时 pDd 更高(中位数[IQR]:1.4[0.6-5.5]比 0.6[0.4-1.2]μg/ml;p<0.0001)和血小板计数(中位数[IQR]:208[158-289]比 189[148-245]×10/L;p = 0.0013)。pDd 截断值为 1.1μg/ml 时,对住院 VTE 的特异性为 72%,灵敏度为 49%,阳性预测值(PPV)为 4%,阴性预测值(NPV)为 99%。截断值为 4.7μg/ml 时,特异性为 95%,灵敏度为 27%,PPV 为 9%,NPV 为 98%。总死亡率与 pDd 值成正比,根据抗凝强度,每个 pDd 类别中的发生率最低:pDd>1.0μg/ml 且接受预防性剂量治疗的患者为 26.3%(p<0.0001),pDd>2.0μg/ml 且接受中等剂量治疗的患者为 28.8%(p = 0.0001),pDd>3.0μg/ml 且接受全剂量抗凝治疗的患者为 31.3%(p = 0.0183)。
在住院的 COVID-19 患者中,pDd 值大于 3.0μg/ml 可用于筛查 VTE 并考虑全剂量抗凝治疗。