Department of Nuclear Medicine, Post Graduate Institute of Medical Education and Research, Chandigarh, India.
Department of Radiotherapy, Post Graduate Institute of Medical Education and Research, Chandigarh, India.
JCO Glob Oncol. 2021 Jul;7:1167-1175. doi: 10.1200/GO.21.00103.
To compare the efficacy and safety of Lu-DOTATATE plus radiosensitizing capecitabine and octreotide long-acting release (LAR) as first-line systemic therapy in advanced well-differentiated gastroenteropancreatic neuroendocrine tumors (GEP-NETs).
Data of consecutive patients of advanced inoperable or metastatic grade 1 or 2 GEP-NETs treated with first-line Lu-DOTATATE plus radiosensitizing capecitabine or octreotide LAR from September 2012 to December 2019 were collected and analyzed for response, toxicity, and survival outcomes.
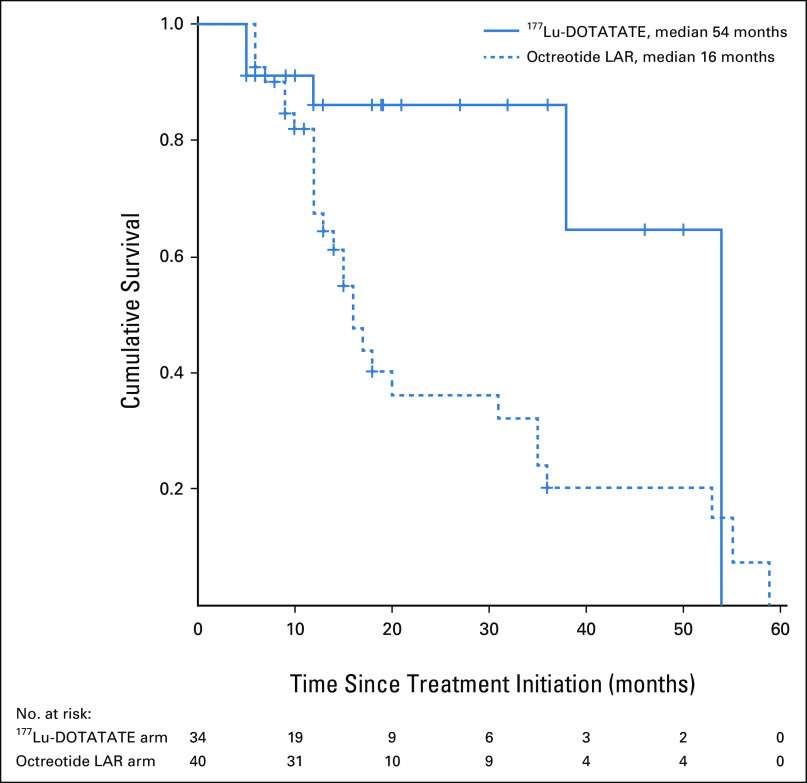
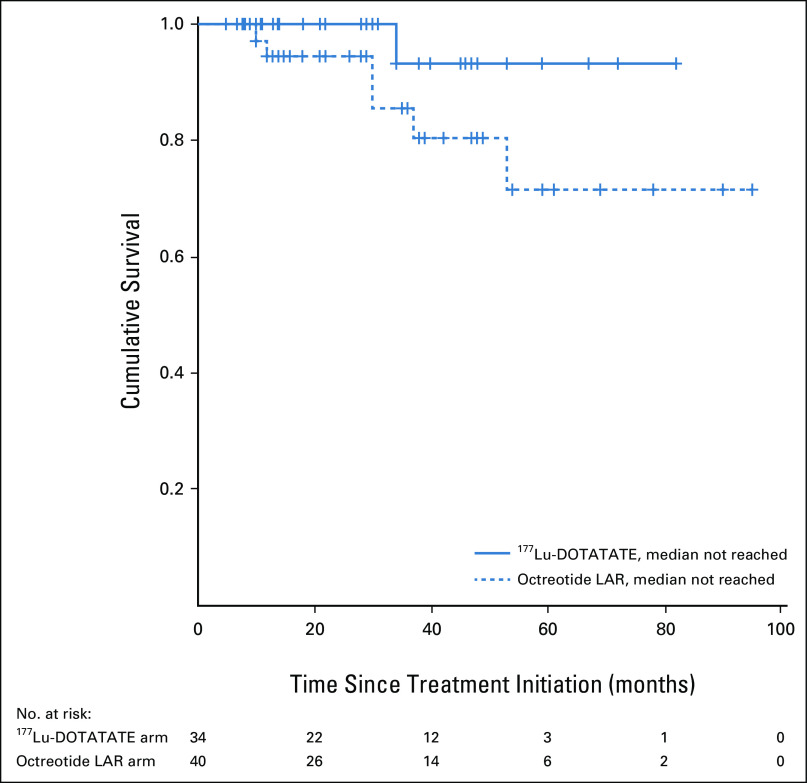
Seventy-six patients (median age: 53 years; range 14-81 years) with treatment-naïve advanced grade 1 or 2 GEP-NETs were included. Thirty-six patients received a median cumulative dose of 27.3 GBq of Lu-DOTATATE intravenously at 8-12 weeks' intervals along with 1,250 mg/m oral capecitabine on days 0-14 of each cycle of Lu-DOTATATE, whereas 40 patients were administered 30 mg octreotide LAR intramuscularly every 4 weeks. Using response evaluation criteria in solid tumor 1.1, the objective response rate was 38% in the Lu-DOTATATE arm compared with 15% in the octreotide LAR arm ( = .025), whereas the disease control rates were 88% and 67% in Lu-DOTATATE and octreotide LAR arms, respectively ( = .035). The median durations of progression-free survival in the Lu-DOTATATE and octreotide LAR arms were 54 months and 16 months, respectively ( = .017), whereas the median overall survival was not reached and not significantly different across both the arms. Of the treatment-related adverse events, no major difference was observed in the occurrence of grade 3 or 4 toxicities between the two treatment arms.
First-line systemic Lu-DOTATATE plus radiosensitizing capecitabine achieved better radiologic response and longer progression-free survival compared with octreotide LAR in patients with advanced grade 1 or 2 GEP-NETs. Future randomized controlled trials are, however, required to determine the best treatment sequence for the treatment-naïve patients with advanced GEP-NETs.
比较 Lu-DOTATATE 联合增敏卡培他滨与奥曲肽长效释放剂(LAR)作为晚期高分化胃肠胰神经内分泌肿瘤(GEP-NETs)一线全身治疗的疗效和安全性。
收集 2012 年 9 月至 2019 年 12 月期间,连续接受一线 Lu-DOTATATE 联合增敏卡培他滨或奥曲肽 LAR 治疗的不可切除或转移性 1 级或 2 级 GEP-NETs 患者的资料,并进行分析,评估其反应、毒性和生存结局。
76 例(中位年龄 53 岁;年龄 14-81 岁)初治晚期 1 级或 2 级 GEP-NETs 患者入组。36 例患者每 8-12 周静脉注射 27.3GBq 的 Lu-DOTATATE,同时在每个 Lu-DOTATATE 周期的第 0-14 天口服 1250mg/m 的卡培他滨,而 40 例患者每 4 周肌内注射 30mg 奥曲肽 LAR。根据实体瘤反应评价标准 1.1,Lu-DOTATATE 组的客观缓解率为 38%,奥曲肽 LAR 组为 15%( =.025),疾病控制率分别为 88%和 67%( =.035)。Lu-DOTATATE 组和奥曲肽 LAR 组的中位无进展生存期分别为 54 个月和 16 个月( =.017),而中位总生存期在两组之间未达到且无显著差异。在治疗相关不良反应方面,两组间 3 级或 4 级毒性的发生率无显著差异。
在晚期 1 级或 2 级 GEP-NETs 患者中,Lu-DOTATATE 联合增敏卡培他滨一线全身治疗较奥曲肽 LAR 获得更好的影像学反应和更长的无进展生存期。然而,需要进一步的随机对照试验来确定初治晚期 GEP-NETs 患者的最佳治疗顺序。