Naeem Faiza, Khan Saira Elaine Anwer, Saeed Muhammad Ahmed, Farman Sumaira
Faiza Naeem, FCPS Internal Medicine, Rheumatology Fellow, Division of Rheumatology, Fatima Memorial Hospital College of Medicine & Dentistry (FMH), Lahore, Pakistan.
Saira E.A Khan, MRCP (UK), SCE Rheumatology (UK) Assistant Professor, Division of Rheumatology, Fatima Memorial Hospital College of Medicine & Dentistry (FMH), Lahore, Pakistan.
Pak J Med Sci. 2021 Jul-Aug;37(4):1001-1007. doi: 10.12669/pjms.37.4.3471.
To identify factors causing diagnostic and therapeutic delay in patients with rheumatoid arthritis, and to evaluate relationship of diagnostic and therapeutic delay with disease outcome.
This cross-sectional study was conducted in Rheumatology Department, Fatima Memorial Hospital, Lahore, Pakistan, from May 2018 to July 2018. In this study 102 patients fulfilling ACR/EULAR criteria 2010 were enrolled. Lag times were calculated in months: lag-1 (delay in initial medical consultation); lag-2 (delay in consulting rheumatologists); lag-3 (diagnostic delay); lag-4 (therapeutic delay). Disease activity and functional outcome were measured by DAS28, HAQ-DI respectively. Association of lag-3 and lag-4 with HAQ-DI and DAS28 was calculated by Pearson correlation.
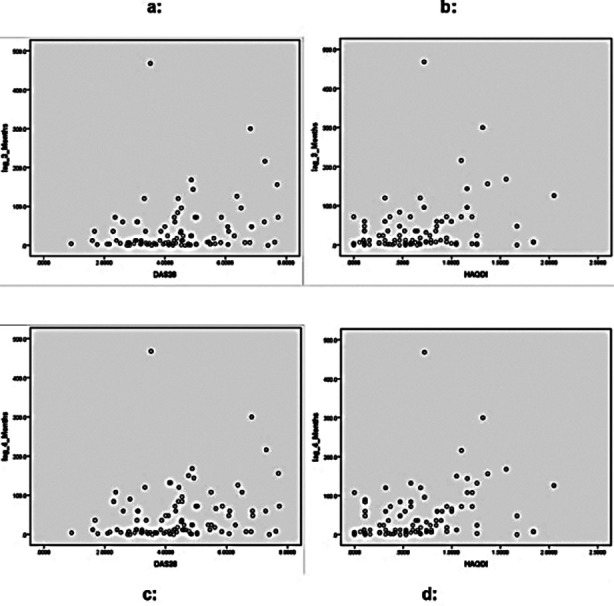
Median (IQR) disease duration of study group was 6(2-10) years. Initial consultations were with; orthopedic surgeon 40(39.2%), general practitioner 27(26.5%), rheumatologist 13(12.7%), medical specialists 14(13.7%). Median (IQR) lag times in months: lag-1 (delayed initial consultation): 2(0-5), lag-2 (delay in consulting rheumatologist): 30(7.7-72), lag-3 (diagnostic delay): 12(3-48), lag-4 (therapeutic delay):18(5.7-72). Factors attributed to lag-3 (diagnostic delay) and lag-4 (therapeutic delay) (p<0.05): older Age (r= 0.2), education level(r= - 0.2), initial consultation (non-rheumatologist) (r=0.2), lag-2(r=0.8), >three doctors visited before diagnosis(r=0.6). Positive anti-CCP antibodies(r=0.2) and lag-1 (delayed initial consultation) (r=1) were associated with lag-3 (diagnostic delay) only; no association was found with positive RA factor. Significant correlation (p=<0.05) of lag-3 (diagnostic delay) was found with both DAS28(r=0.2) & HAQ-DI(r=0.2). Similarly lag-4 (therapeutic delay) also correlated with both & DAS28(r=0.2) & HAQ-DI(r=0.3) (p=<0.05).
Diagnostic and therapeutic delay were associated with older age, lower education and delayed consultation with rheumatologist but not with positive RA factor. Positive anti-CCP antibodies were associated with diagnostic delay only. Diagnostic and therapeutic delay led to high disease activity and poor functional outcome in RA patients.
确定导致类风湿关节炎患者诊断和治疗延迟的因素,并评估诊断和治疗延迟与疾病结局的关系。
这项横断面研究于2018年5月至2018年7月在巴基斯坦拉合尔法蒂玛纪念医院风湿科进行。本研究纳入了102例符合2010年美国风湿病学会/欧洲抗风湿病联盟(ACR/EULAR)标准的患者。延迟时间以月计算:延迟-1(初次就医延迟);延迟-2(咨询风湿病学家延迟);延迟-3(诊断延迟);延迟-4(治疗延迟)。分别通过28个关节疾病活动评分(DAS28)、健康评估问卷残疾指数(HAQ-DI)来测量疾病活动度和功能结局。通过Pearson相关性分析计算延迟-3和延迟-4与HAQ-DI和DAS28之间的关联。
研究组的疾病持续时间中位数(四分位间距)为6(2 - 10)年。初次就诊的医生为:骨科医生40例(39.2%)、全科医生27例(26.5%)、风湿病学家13例(12.7%)、内科专家14例(13.7%)。延迟时间中位数(四分位间距)(以月计):延迟-1(初次就医延迟):2(0 - 5),延迟-2(咨询风湿病学家延迟):30(7.7 - 72),延迟-3(诊断延迟):12(3 - 48),延迟-4(治疗延迟):18(5.7 - 72)。归因于延迟-3(诊断延迟)和延迟-4(治疗延迟)的因素(p<0.05):年龄较大(r = 0.2)、教育水平(r = - 0.2)、初次就诊(非风湿病学家)(r = 0.2)、延迟-2(r = 0.8)、诊断前就诊医生>3名(r = 0.6)。抗环瓜氨酸肽(CCP)抗体阳性(r = 0.2)和延迟-1(初次就医延迟)(r = 1)仅与延迟-3(诊断延迟)相关;未发现与类风湿因子阳性有关联。发现延迟-3(诊断延迟)与DAS28(r = 0.2)和HAQ-DI(r = 0.2)均存在显著相关性(p =<0.05)。同样,延迟-4(治疗延迟)也与DAS28(r = 0.2)和HAQ-DI(r = 0.3)相关(p =<0.05)。
诊断和治疗延迟与年龄较大、教育程度较低以及咨询风湿病学家延迟有关,但与类风湿因子阳性无关。抗CCP抗体阳性仅与诊断延迟有关。诊断和治疗延迟导致类风湿关节炎患者疾病活动度高且功能结局差。