Pasini Andrea, Bertulli Cristina, Casadio Luca, Corrado Ciro, Edefonti Alberto, Ghiggeri GianMarco, Ghio Luciana, Giordano Mario, La Scola Claudio, Malaventura Cristina, Maringhini Silvio, Mastrangelo Antonio P, Materassi Marco, Mencarelli Francesca, Messina Giovanni, Monti Elena, Morello William, Puccio Giuseppe, Romagnani Paola, Montini Giovanni
Nephrology and Dialysis Unit, Department of Pediatrics, IRCCS Azienda Ospedaliero-Universitaria di Bologna, Bologna, Italy.
Unità Operativa Complessa of Paediatrics and Neonatology, Local Health Authority of Romagna, Ravenna, Italy.
Front Pediatr. 2021 Jul 8;9:627636. doi: 10.3389/fped.2021.627636. eCollection 2021.
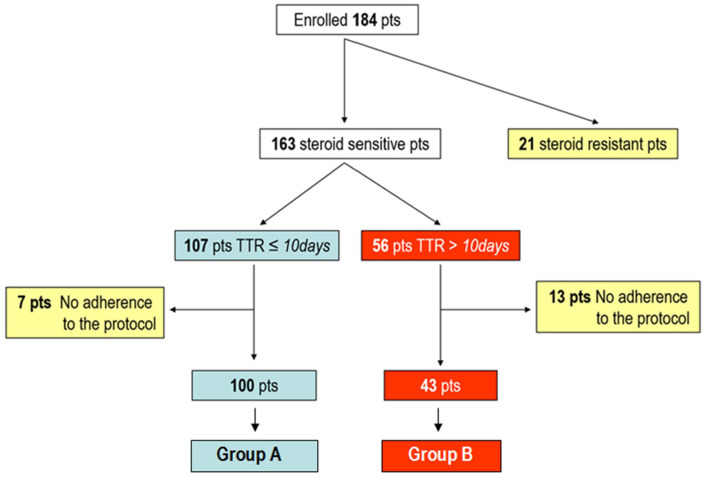
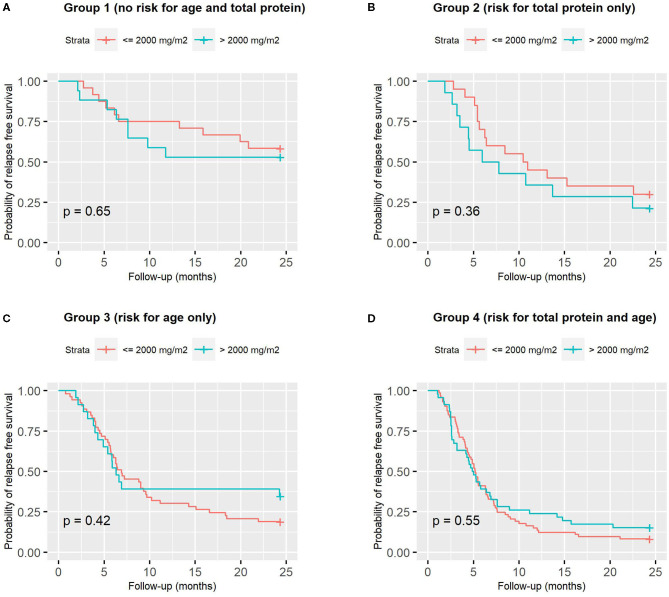
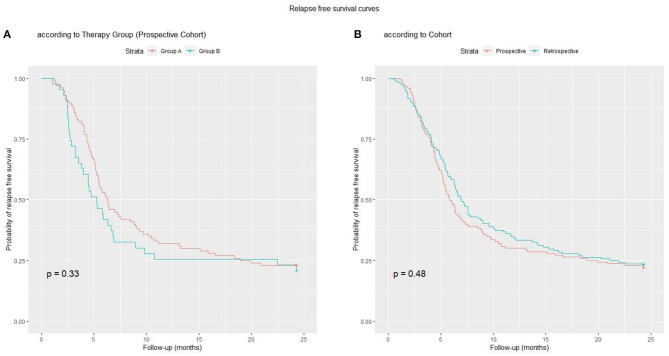
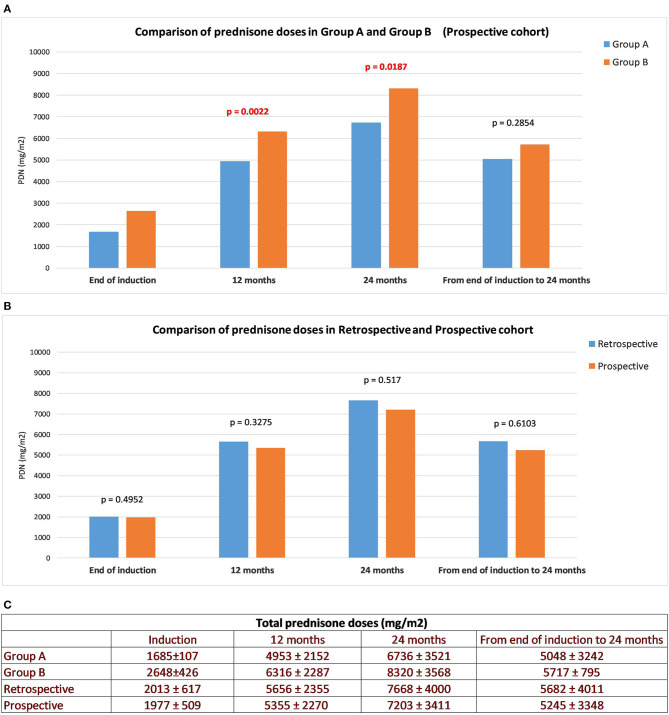
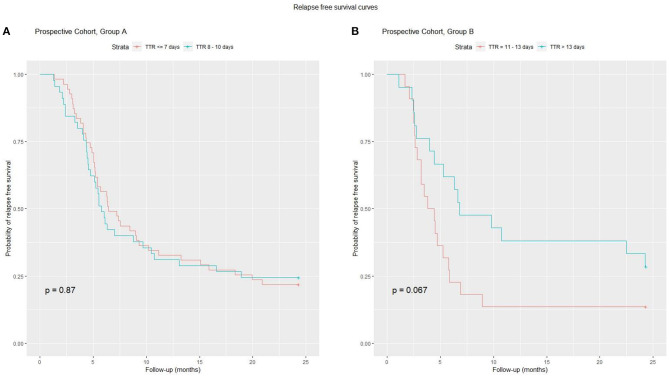
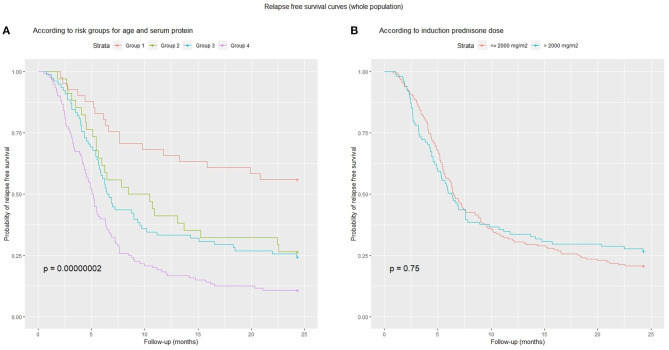
A great majority of children with idiopathic nephrotic syndrome will relapse after successful treatment of the initial episode. The possibility that different steroid dosing regimens at onset, adjusted for risk factors, can reduce the rate of relapse represents an interesting option to investigate. To evaluate the effect of the initial steroid regimen, adjusted for time to remission (TTR), on the frequency of relapses and steroid dependence, and to verify the influence of prognostic factors on disease course. A multicentre, prospective, cohort study. Children with nephrotic syndrome, with TTR ≤ 10 days (Group A), were given a 20-week prednisone regimen (2,828 mg/m) and those with a TTR >10 days, a 22-week regimen (3,668 mg/m) (Group B). Previously published retrospective data from the same centers were also evaluated. Main outcomes were: relapse rate, number of frequent relapsers + steroid dependent children and total prednisone dose after induction. 143 children were enrolled. Rate of relapsed subjects (77 vs. 79%) and frequent relapsers + steroid dependent subjects (40 vs. 53%) did not differ between Groups A and B, or between the retrospective and prospective cohorts. The cumulative prednisone dose taken after the induction treatment was similar in both groups and in the retrospective and prospective cohorts. TTR was not associated with relapse risk. Age at onset and total serum protein were significantly lower in relapsing patients. At ROC analysis, the best cut-off was 5.3 years for age at onset and 4.2 g/dL for total serum protein. According to these cut-offs, older children with higher total serum protein had a higher relapse free survival rate (58%) than younger children with lower total serum protein (17%). TTR was not found to be a prognostic factor of relapse; because of this, different steroid regimens, adjusted for TTR, did not modify the relapse rate in any relevant measure. Conversely, younger age and low total serum protein were independent predictors of relapse risk, however this outcome was not modified by higher prednisone regimens. https://www.ClinicalTrials.gov/, identifier: NCT01386957 (www.nefrokid.it).
绝大多数特发性肾病综合征患儿在初次发作成功治疗后会复发。针对风险因素调整起始时不同的类固醇给药方案能否降低复发率,这是一个值得研究的有趣选项。为评估根据缓解时间(TTR)调整的初始类固醇方案对复发频率和类固醇依赖的影响,并验证预后因素对疾病进程的影响。一项多中心、前瞻性队列研究。肾病综合征患儿中,TTR≤10天的患儿(A组)接受20周的泼尼松方案(2828mg/m),TTR>10天的患儿接受22周的方案(3668mg/m)(B组)。还评估了来自同一中心之前发表的回顾性数据。主要结局指标为:复发率、频繁复发者+类固醇依赖患儿的数量以及诱导后泼尼松的总剂量。共纳入143名患儿。A组和B组之间,以及回顾性队列和前瞻性队列之间,复发受试者的比例(77%对79%)和频繁复发者+类固醇依赖受试者的比例(40%对53%)并无差异。诱导治疗后两组以及回顾性队列和前瞻性队列中泼尼松的累积剂量相似。TTR与复发风险无关。复发患者的发病年龄和总血清蛋白显著更低。在ROC分析中,发病年龄的最佳截断值为5.3岁,总血清蛋白的最佳截断值为4.2g/dL。根据这些截断值,总血清蛋白较高的大龄儿童无复发生存率(58%)高于总血清蛋白较低的小龄儿童(17%)。未发现TTR是复发的预后因素;因此,根据TTR调整的不同类固醇方案在任何相关指标上均未改变复发率。相反,低龄和低总血清蛋白是复发风险的独立预测因素,然而更高的泼尼松方案并未改变这一结果。https://www.ClinicalTrials.gov/,标识符:NCT01386957(www.nefrokid.it)