Yang Camerdy Yue, Tsai Sheng-Ta
Department of Neurology, China Medical University Hospital, Taichung 404332, Taiwan.
World J Clin Cases. 2021 Jul 6;9(19):5325-5331. doi: 10.12998/wjcc.v9.i19.5325.
Anti-glutamic acid decarboxylase (GAD) antibody is known to cause several autoimmune-related situations. The most known relationship is that it may cause type I diabetes. In addition, it was also reported to result in several neurologic syndromes including stiff person syndrome, cerebellar ataxia, and autoimmune encephalitis. Decades ago, isolated epilepsy associated with anti-GAD antibody was first reported. Recently, the association between temporal lobe epilepsy and anti-GAD antibody has been discussed. Currently, with improvements in examination technique, many more autoimmune-related disorders can be diagnosed and treated easier than in the past.
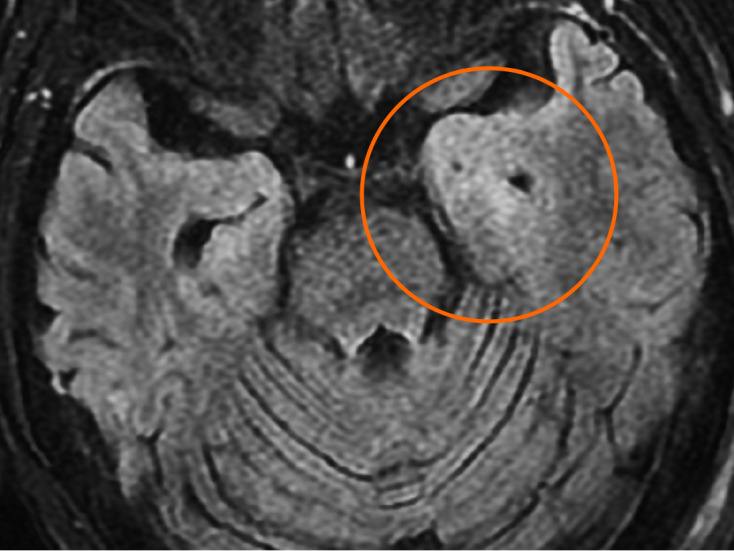
A 44-year-old female Asian with a history of end-stage renal disease (without diabetes mellitus) under hemodialysis presented with diffuse abdominal pain. The initial diagnosis was peritonitis complicated with sepsis and paralytic ileus. Her peritonitis was treated and she recovered well, but seizure attack was noticed during hospitalization. The clinical impression was gelastic seizure with the presentation of frequent smiling, head turned to the right side, and eyes staring without focus; the duration was about 5-10 s. Temporal lobe epilepsy was recorded through electroencephalogram, and she was later diagnosed with anti-GAD65 antibody positive autoimmune encephalitis. Her seizure was treated initially with several anticonvulsants but with poor response. However, she showed excellent response to intravenous methylprednisolone pulse therapy. Her consciousness returned to normal, and no more seizures were recorded after 5 d of intravenous methylprednisolone treatment.
In any case presenting with new-onset epilepsy, in addition to performing routine brain imaging to exclude structural lesion and cerebrospinal fluid studies to exclude common etiologies of infection and inflammation, checking the autoimmune profile has to be considered. In the practice of modern medicine, autoimmune-related disorders are relatively treatable and should not be missed.
抗谷氨酸脱羧酶(GAD)抗体已知会引发多种自身免疫相关情况。最广为人知的关系是它可能导致I型糖尿病。此外,据报道它还会引发多种神经综合征,包括僵人综合征、小脑共济失调和自身免疫性脑炎。几十年前,首次报道了与抗GAD抗体相关的孤立性癫痫。最近,颞叶癫痫与抗GAD抗体之间的关联也受到了讨论。目前,随着检查技术的进步,比起过去,更多自身免疫相关疾病能够被诊断和治疗。
一名44岁的亚洲女性,有终末期肾病病史(无糖尿病),正在接受血液透析,出现弥漫性腹痛。初步诊断为腹膜炎合并败血症和麻痹性肠梗阻。她的腹膜炎得到了治疗,恢复良好,但住院期间出现了癫痫发作。临床印象为痴笑发作,表现为频繁微笑、头转向右侧、双眼凝视无焦点;持续时间约5 - 10秒。通过脑电图记录为颞叶癫痫,后来她被诊断为抗GAD65抗体阳性自身免疫性脑炎。她的癫痫最初用几种抗惊厥药治疗,但效果不佳。然而,她对静脉注射甲泼尼龙冲击疗法反应良好。静脉注射甲泼尼龙治疗5天后,她的意识恢复正常,未再出现癫痫发作。
对于任何新发癫痫的病例,除了进行常规脑部影像学检查以排除结构性病变以及脑脊液检查以排除感染和炎症的常见病因外,还必须考虑检查自身免疫指标。在现代医学实践中,自身免疫相关疾病相对可治,不应被漏诊。