Department of Neurosurgery, Hirosaki University Graduate School of Medicine, 5 Zaifu-cho, Hirosaki, Aomori, 036-8562, Japan.
Clinical Research Support Center, Hirosaki University Hospital, 53 Hon-cho, Hirosaki, Aomori, 036-8563, Japan.
BMC Cancer. 2021 Jul 28;21(1):867. doi: 10.1186/s12885-021-08592-z.
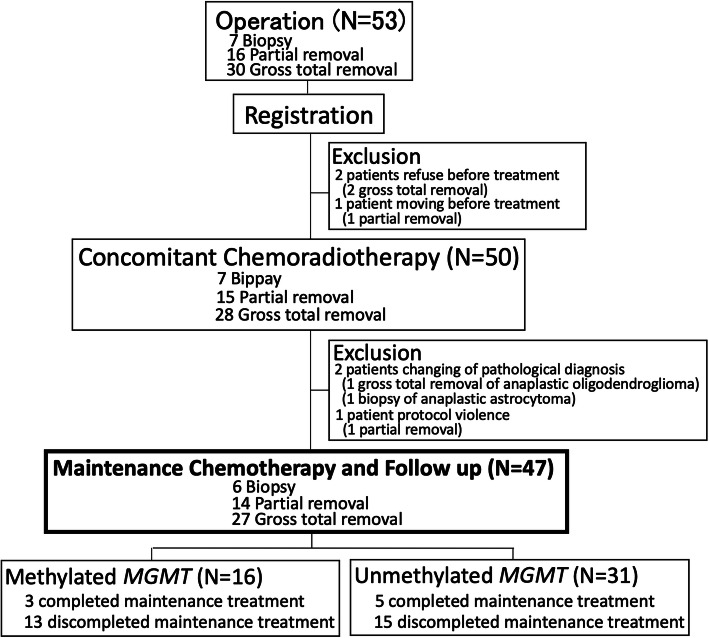
This investigator-initiated, open-label, single-arm, single-institute study was conducted to investigate the effectiveness of induction combination chemoradiotherapy and long-term maintenance therapy with temozolomide (TMZ) plus interferon (IFN)-β for glioblastoma.
The initial induction combination chemoradiotherapy comprised radiotherapy plus TMZ plus vincristine plus IFN-β. Maintenance chemotherapy comprised monthly TMZ, continued for 24-50 cycles, plus weekly IFN-β continued for as long as possible. The primary endpoint was 2-year overall survival (2y-OS). The study protocol was to be considered valid if the expected 2y-OS was over 38% and the lower limit of the 95% confidence interval (CI) was no less than 31.7% compared with historical controls, using Kaplan-Meier methods. Secondary endpoints were median progression-free survival (mPFS), median OS (mOS), 5-year OS rate (5y-OS), and mPFS and mOS classified according to MGMT promoter methylation status.
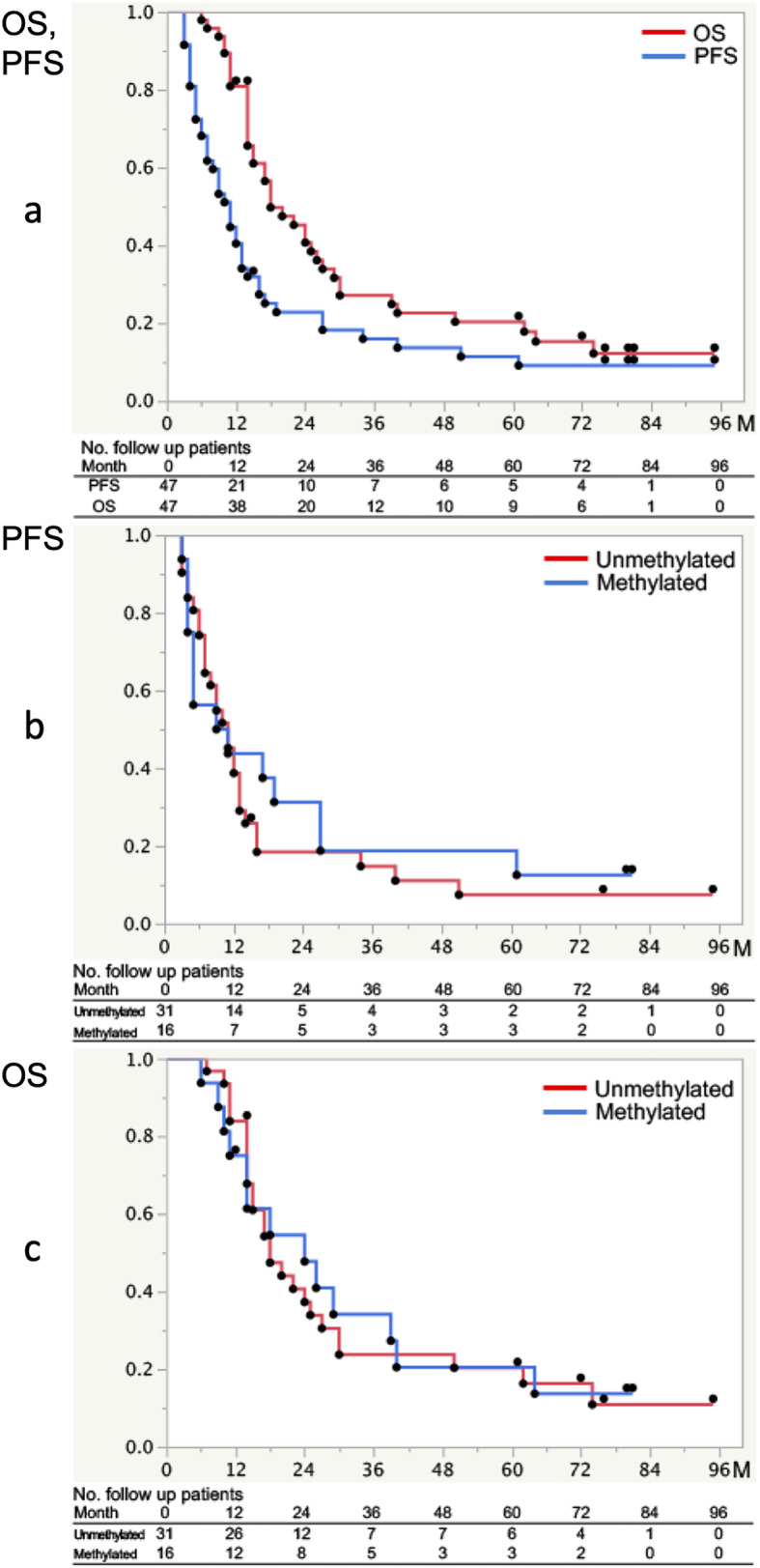
Forty-seven patients were analyzed. The 2y-OS was 40.7% (95%CI, 27.5-55.4%). The mPFS and mOS were 11.0 months and 18.0 months, respectively, and 5y-OS was 20.3% (95%CI, 10.9-34.6%). The mPFS in groups with and without MGMT promoter methylation in the tumor was 10.0 months and 11.0 months (p = 0.59), respectively, and mOS was 24.0 months and 18.0 months (p = 0.88), respectively. The frequency of grade 3/4 neutropenia was 19.1%.
The 2y-OS with induction multidrug combination chemoradiotherapy and long-term maintenance therapy comprising TMZ plus IFN-β tended to exceed that of historical controls, but the lower limit of the 95%CI was below 31.7%. Although the number of cases was small, this protocol may rule out MGMT promoter methylation status as a prognostic factor.
University Hospital Medical Information Network (number UMIN000040599 ).
本研究为研究者发起的、开放性、单臂、单中心研究,旨在探究替莫唑胺(TMZ)联合干扰素(IFN)-β诱导联合放化疗和长期维持治疗胶质母细胞瘤的疗效。
初始诱导联合放化疗方案为放疗+TMZ+长春新碱+IFN-β。维持化疗方案为每月 TMZ 联合治疗,持续 24-50 个周期,每周 IFN-β持续使用至尽可能长的时间。主要终点为 2 年总生存率(2y-OS)。采用 Kaplan-Meier 法,如果预期 2y-OS 超过 38%,95%置信区间(CI)下限不低于 31.7%,与历史对照相比,研究方案即被认为有效。次要终点为无进展生存期(mPFS)、总生存期(mOS)、5 年生存率(5y-OS),以及根据 MGMT 启动子甲基化状态分类的 mPFS 和 mOS。
共 47 例患者纳入分析。2y-OS 为 40.7%(95%CI,27.5-55.4%)。mPFS 和 mOS 分别为 11.0 个月和 18.0 个月,5y-OS 为 20.3%(95%CI,10.9-34.6%)。肿瘤中存在和不存在 MGMT 启动子甲基化的患者 mPFS 分别为 10.0 个月和 11.0 个月(p=0.59),mOS 分别为 24.0 个月和 18.0 个月(p=0.88)。3/4 级中性粒细胞减少症发生率为 19.1%。
与历史对照相比,诱导多药联合放化疗联合 TMZ 联合 IFN-β长期维持治疗的 2y-OS 有升高趋势,但 95%CI 的下限低于 31.7%。尽管病例数较少,但该方案可能排除 MGMT 启动子甲基化状态作为预后因素。
大学医院医疗信息网络(编号 UMIN000040599)。