Department of Thoracic and Cardiovascular Surgery, Herz- und Diabeteszentrum NRW, University Hospital Ruhr-University Bochum, Bad Oeynhausen, Germany.
Department of Cardiovascular Surgery, Heart Center Duisburg, Duisburg, Germany.
Interact Cardiovasc Thorac Surg. 2021 Nov 22;33(6):857-865. doi: 10.1093/icvts/ivab179.
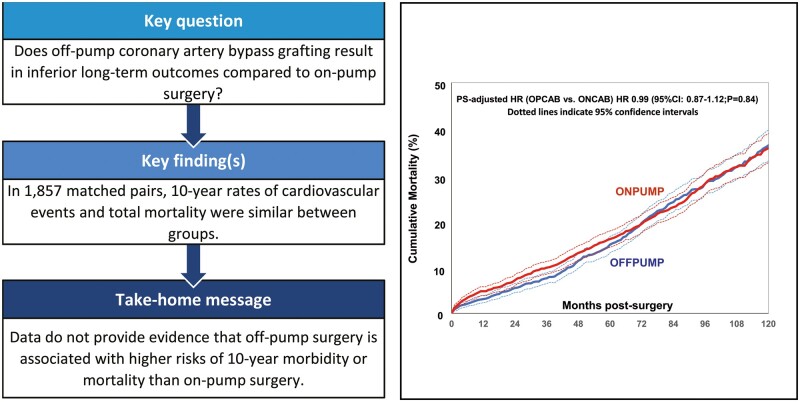
Recent data suggested that off-pump coronary artery bypass (OPCAB) may carry a higher risk for mortality in the long term when compared to on-pump coronary artery bypass (ONCAB). We, therefore, compared long-term survival and morbidity in patients undergoing ONCAB versus OPCAB in a large single-centre cohort.
A total of 8981 patients undergoing isolated elective/urgent coronary artery bypass grafting between January 2009 and December 2019 were analysed. Patients were stratified into 2 groups (OPCAB n = 6649/ONCAB n = 2332). The primary end point was all-cause mortality. Secondary endpoints included repeat revascularization, stroke and myocardial infarction. To adjust for potential selection bias, 1:1 nearest neighbour propensity score (PS) matching was performed resulting in 1857 matched pairs. Moreover, sensitivity analysis was applied in the entire study cohort using multivariable- and PS-adjusted Cox regression analysis.
In the PS-matched cohort, 10-year mortality was similar between study groups [OPCAB 36.4% vs ONCAB 35.8%: hazard ratio (HR) 0.99, 95% confidence interval (CI) 0.87-1.12; P = 0.84]. While 10-year outcomes of secondary endpoints did not differ significantly, risk of stroke (OPCAB 1.50% vs ONCAB 2.8%: HR 0.51, 95% CI 0.32-0.83; P = 0.006) and mortality (OPCAB 3.1% vs ONCAB 4.8%: HR 0.65, 95% CI 0.47-0.91; P = 0.011) at 1 year was lower in the OPCAB group. In the multivariable- and the PS-adjusted model, mortality at 10 years was not significantly different (OPCAB 34.1% vs ONCAB 35.7%: HR 0.97, 95% CI 0.87-1.08; P = 0.59 and HR 1.01, 95% CI 0.90-1.13; P = 0.91, respectively).
Data do not provide evidence that elective/urgent OPCAB is associated with significantly higher risks of mortality, repeat revascularization, or myocardial infarction during late follow-up when compared to ONCAB. Patients undergoing OPCAB may benefit from reduced risks of stroke and mortality within the first year postoperatively.
最近的数据表明,与体外循环冠状动脉旁路移植术(ONCAB)相比,非体外循环冠状动脉旁路移植术(OPCAB)在长期内的死亡率更高。因此,我们在一个大型单中心队列中比较了接受 ONCAB 与 OPCAB 的患者的长期生存和发病率。
分析了 2009 年 1 月至 2019 年 12 月期间接受择期/紧急冠状动脉旁路移植术的 8981 例患者。患者分为 2 组(OPCAB n=6649/ONCAB n=2332)。主要终点为全因死亡率。次要终点包括再次血运重建、卒中和心肌梗死。为了调整潜在的选择偏倚,采用 1:1 最近邻居倾向评分(PS)匹配,得到 1857 对匹配。此外,在整个研究队列中应用多变量和 PS 调整的 Cox 回归分析进行敏感性分析。
在 PS 匹配的队列中,两组患者的 10 年死亡率相似[OPCAB 组为 36.4%,ONCAB 组为 35.8%:风险比(HR)0.99,95%置信区间(CI)0.87-1.12;P=0.84]。虽然次要终点的 10 年结局无显著差异,但 OPCAB 组的卒中风险(OPCAB 组 1.50%,ONCAB 组 2.8%:HR 0.51,95%CI 0.32-0.83;P=0.006)和死亡率(OPCAB 组 3.1%,ONCAB 组 4.8%:HR 0.65,95%CI 0.47-0.91;P=0.011)在 1 年时较低。在多变量和 PS 调整的模型中,10 年死亡率无显著差异(OPCAB 组为 34.1%,ONCAB 组为 35.7%:HR 0.97,95%CI 0.87-1.08;P=0.59 和 HR 1.01,95%CI 0.90-1.13;P=0.91)。
数据并未表明择期/紧急 OPCAB 与 ONCAB 相比,在晚期随访期间死亡率、再次血运重建或心肌梗死的风险显著增加。接受 OPCAB 的患者可能在术后 1 年内受益于降低的卒中风险和死亡率。