Buisson Anthony, Cannon Lisa, Umanskiy Konstantin, Hurst Roger D, Hyman Neil H, Sakuraba Atsushi, Pekow Joel, Dalal Sushila, Cohen Russell D, Pereira Bruno, Rubin David T
Inflammatory Bowel Disease Center, University of Chicago Medicine, Chicago, IL, USA.
Inflammatory Bowel Unit, Inserm, 3iHP, CHU Clermont-Ferrand, Clermont Auvergne University, Clermont-Ferrand, France.
Intest Res. 2022 Jul;20(3):303-312. doi: 10.5217/ir.2021.00018. Epub 2021 Aug 4.
BACKGROUND/AIMS: We assessed the effectiveness of anti-TNF agents and its associated factors to prevent endoscopic and clinical postoperative recurrence (POR) in Crohn's disease (CD).
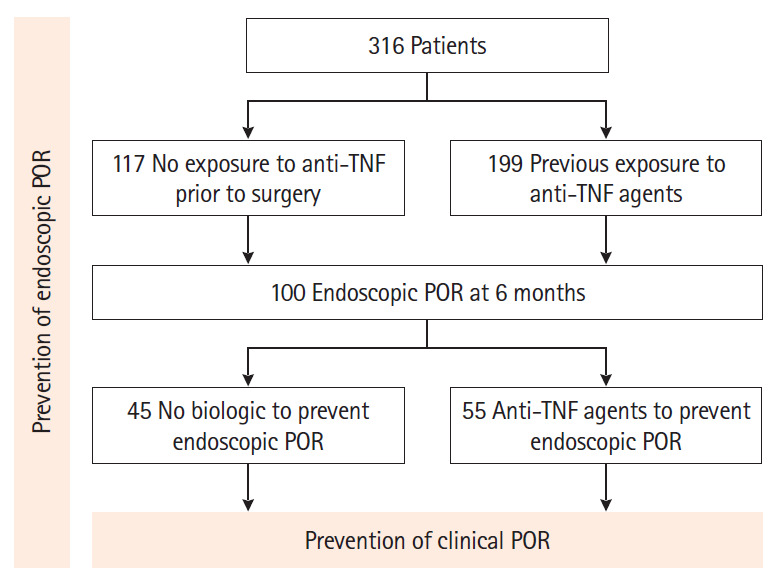
From a prospectively-maintained database, we retrieved 316 CD patients who underwent intestinal resection (2011-2017). Endoscopic (Rutgeerts index ≥ i2 at 6 months) and clinical (recurrence of symptoms leading to hospitalization or therapeutic escalation) POR were assessed.
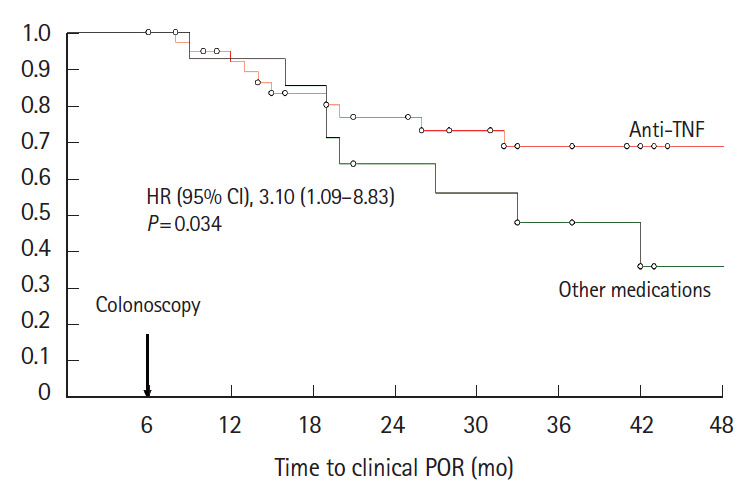
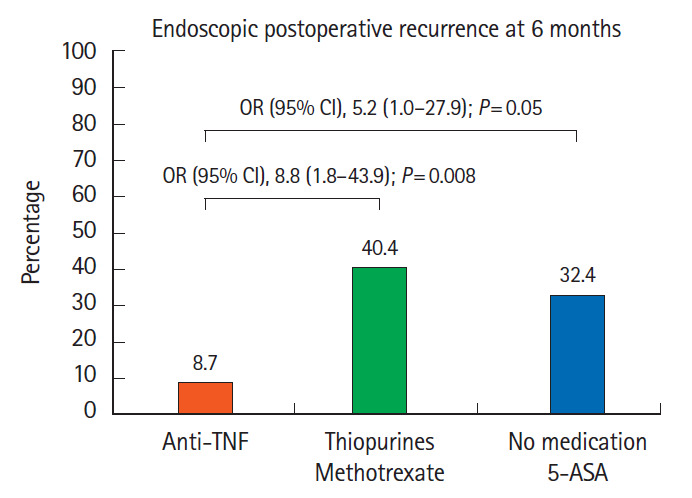
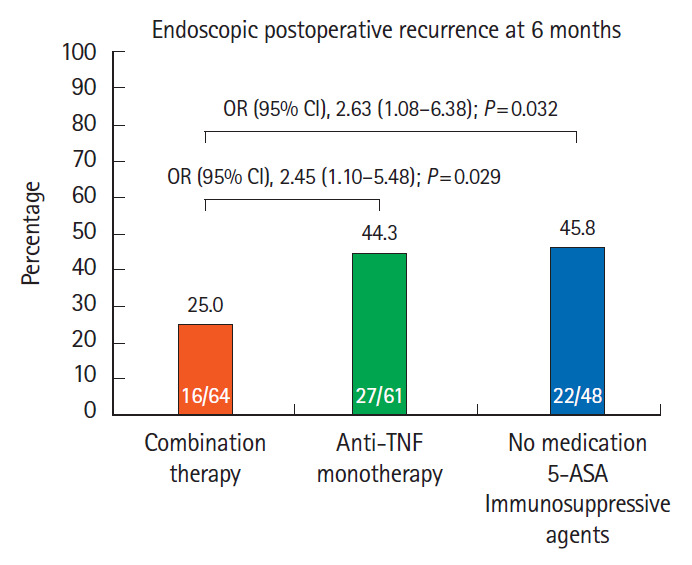
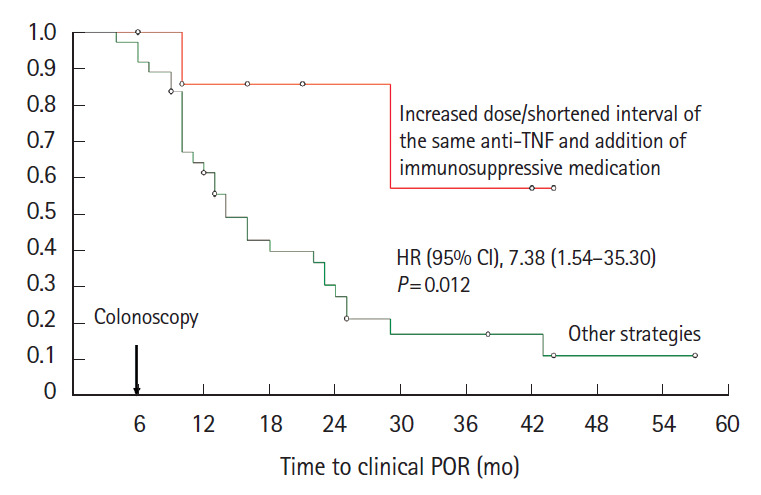
In 117 anti-TNF-naïve patients, anti-TNF therapy was more effective than immunosuppressive agents (odds ratio [OR], 8.8; 95% confidence interval [CI], 1.8-43.9; P= 0.008) and no medication/5-aminosalicylates (OR, 5.2; 95% CI, 1.0-27.9; P= 0.05) to prevent endoscopic POR. In 199 patients exposed to anti-TNF prior to the surgery, combination with anti-TNF and immunosuppressive agents was more effective than anti-TNF monotherapy (OR, 2.32; 95% CI, 1.02-5.31; P= 0.046) to prevent endoscopic POR. Primary failure to anti-TNF agent prior to surgery was predictive of anti-TNF failure to prevent endoscopic POR (OR, 2.41; 95% CI, 1.10-5.32; P= 0.03). When endoscopic POR despite anti-TNF prophylactic medication (n = 55), optimizing anti-TNF and adding an immunosuppressive drug was the most effective option to prevent clinical POR (hazard ratio, 7.38; 95% CI, 1.54-35.30; P= 0.012). Anti-TNF therapy was the best option to prevent clinical POR (hazard ratio, 3.10; 95% CI, 1.09-8.83; P= 0.034) in patients with endoscopic POR who did not receive any biologic to prevent endoscopic POR (n = 55).
Anti-TNF was the most effective medication to prevent endoscopic and clinical POR. Combination with anti-TNF and immunosuppressive agents should be considered in patients previously exposed to anti-TNF.
背景/目的:我们评估了抗TNF药物预防克罗恩病(CD)内镜及临床术后复发(POR)的有效性及其相关因素。
从一个前瞻性维护的数据库中,我们检索了316例接受肠道切除术的CD患者(2011 - 2017年)。评估内镜下(6个月时鲁氏分级指数≥i2)及临床(因症状复发导致住院或治疗升级)POR情况。
在117例未使用过抗TNF药物的患者中,抗TNF治疗在预防内镜下POR方面比免疫抑制剂(优势比[OR],8.8;95%置信区间[CI],1.8 - 43.9;P = 0.008)和未用药/5 - 氨基水杨酸类药物(OR,5.2;95% CI,1.0 - 27.9;P = 0.05)更有效。在199例手术前已接触过抗TNF药物的患者中,抗TNF与免疫抑制剂联合使用在预防内镜下POR方面比抗TNF单药治疗更有效(OR,2.32;95% CI,1.02 - 5.31;P = 0.046)。手术前抗TNF药物原发性失效可预测抗TNF预防内镜下POR失败(OR,2.41;95% CI,1.10 - 5.32;P = 0.03)。当尽管使用抗TNF预防性药物仍发生内镜下POR时(n = 55),优化抗TNF并加用免疫抑制药物是预防临床POR的最有效选择(风险比,7.38;95% CI,1.54 - 35.30;P = 0.012)。在未接受任何生物制剂预防内镜下POR的内镜下POR患者中(n = 55),抗TNF治疗是预防临床POR的最佳选择(风险比,3.10;95% CI,1.09 - 8.83;P = 0.034)。
抗TNF是预防内镜及临床POR最有效的药物。对于既往接触过抗TNF的患者,应考虑抗TNF与免疫抑制剂联合使用。