Coelingh Bennink Herjan J T, van Moorselaar Jeroen A, Crawford E David, Roos Erik P M, Somford Diederik M, Roeleveld Ton A, de Haan Tjard D, van Melick Harm H E, Reisman Yacov, Zimmerman Yvette, van Osta Gonnie, Krijgh Jan, Shore Neal D, Saad Fred, Schally Andrew V, Debruyne Frans M J
Pantarhei Oncology, Zeist, The Netherlands.
Amsterdam UMC, Free University, Amsterdam, The Netherlands.
Eur Urol Open Sci. 2021 May 6;28:52-61. doi: 10.1016/j.euros.2021.04.005. eCollection 2021 Jun.
Androgen deprivation therapy (ADT) for prostate cancer with luteinizing hormone-releasing hormone (LHRH) agonists can be improved.
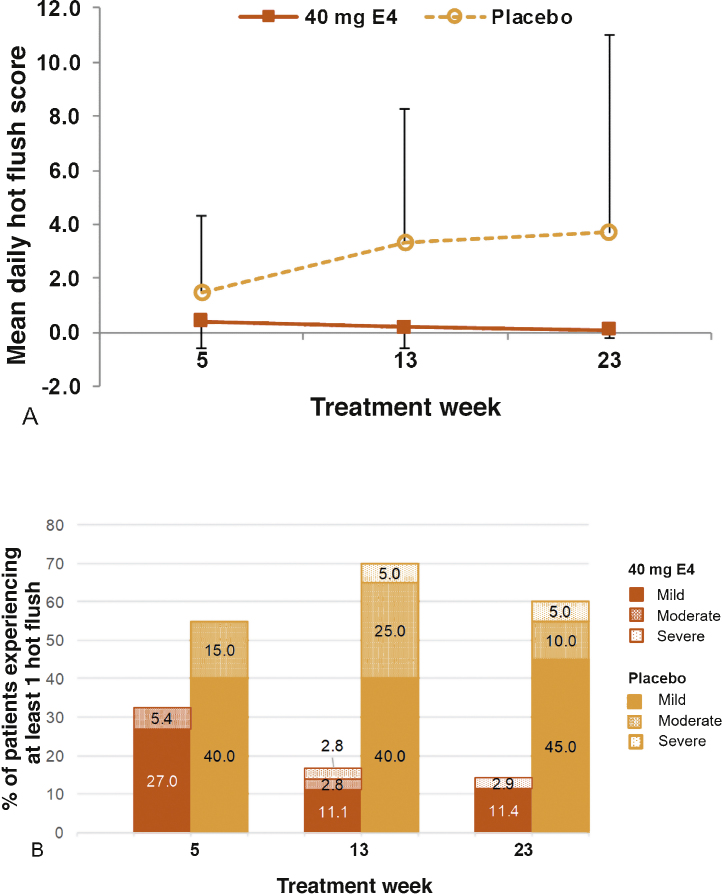
To assess safety, the frequency and severity of hot flushes (HFs), bone health, and antitumor effects of high-dose estetrol (HDE4) when combined with ADT.
A phase II, double-blind, randomized, placebo-controlled study was conducted in advanced prostate cancer patients requiring ADT (the PCombi study).
Patients receiving LHRH agonist treatment were randomized 2:1 to 40 mg HDE4 ( = 41) or placebo ( = 21) cotreatment for 24 wk.
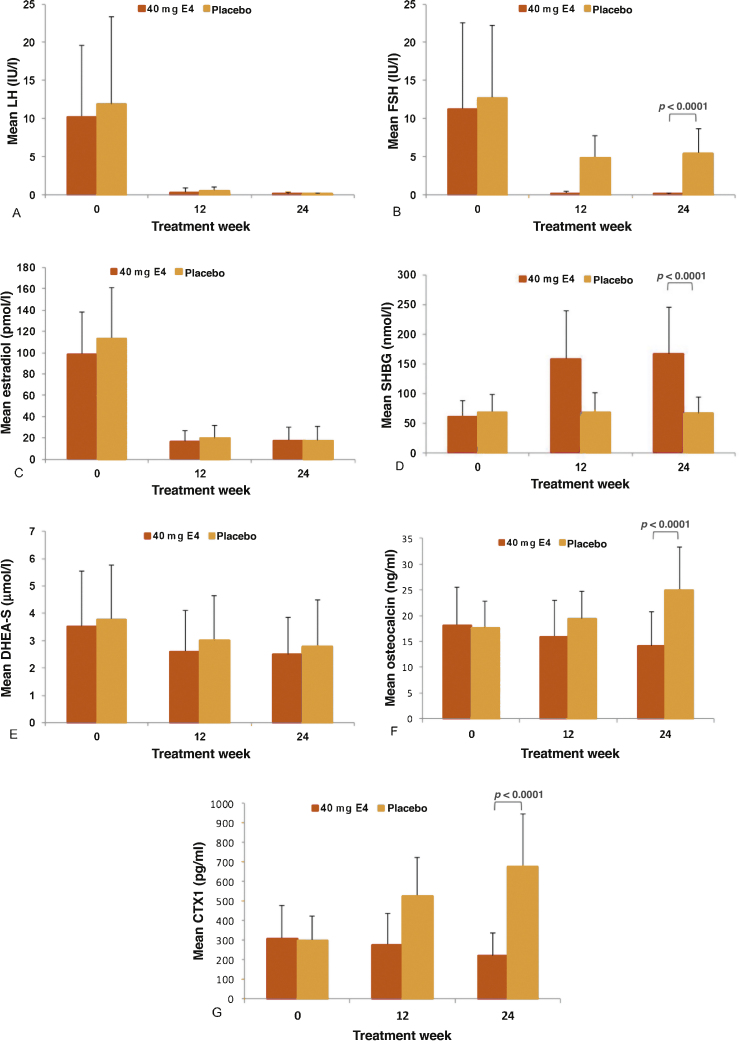
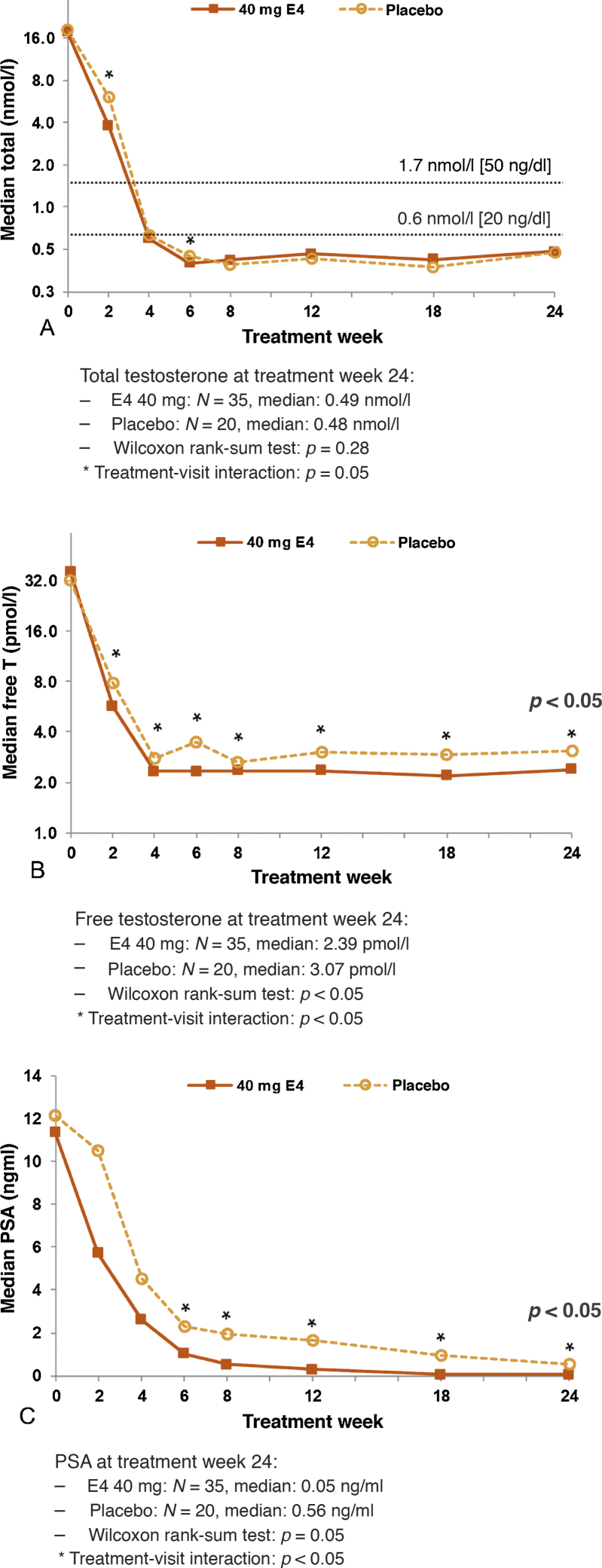
Coprimary endpoints were frequency/severity of HFs and levels of total and free testosterone (T). Secondary endpoints included assessments of bone metabolism (osteocalcin and type I collagen telopeptide [CTX1]), prostate-specific antigen (PSA), and follicle-stimulating hormone (FSH). Efficacy analysis was based on the selected per-protocol (PP) population.
Of 62 patients included in the study, 57 were suitable for a PP analysis (37 HDE4; 20 placebo). No E4-related serious cardiovascular adverse events occurred at 24 wk. Weekly HFs were reported by 13.5% of patients with HDE4 and 60.0% with placebo ( < 0.001). Daily HFs occurred in 5.9% versus 55%. Bone turnover parameters decreased significantly with HDE4 ( < 0.0001). Total and free T decreased earlier ( < 0.05), and free T was suppressed further ( < 0.05). PSA suppression was more profound and earlier ( < 0.005). FSH levels were suppressed by 98% versus 57% ( < 0.0001). Estrogenic side effects were nipple sensitivity (34%) and gynecomastia (17%).
HDE4 cotreatment of ADT patients with advanced prostate cancer was well tolerated, and no treatment-related cardiovascular adverse events were observed at 24 wk. HFs and bone turnover were substantially reduced. Suppression of free T, PSA, and FSH was more rapid and profound, suggesting enhanced disease control by HDE4 cotreatment. Larger and longer-lasting studies are needed to confirm the results of the study reported here.
Cotreatment of androgen deprivation therapy with high-dose estetrol in advanced prostate cancer patients results in fewer occurrences of hot flushes, bone protection, and other antitumor benefits. Nipple sensitivity and gynecomastia may occur as side effects.
用于前列腺癌的促黄体生成素释放激素(LHRH)激动剂雄激素剥夺疗法(ADT)可得到改进。
评估高剂量雌三醇(HDE4)与ADT联合使用时的安全性、潮热(HFs)的频率和严重程度、骨骼健康及抗肿瘤效果。
设计、地点和参与者:在需要ADT的晚期前列腺癌患者中进行了一项II期、双盲、随机、安慰剂对照研究(PCombi研究)。
接受LHRH激动剂治疗的患者按2:1随机分为接受40mg HDE4(n = 41)或安慰剂(n = 21)联合治疗24周。
共同主要终点为HFs的频率/严重程度以及总睾酮和游离睾酮(T)水平。次要终点包括骨代谢(骨钙素和I型胶原末端肽[CTX1])、前列腺特异性抗原(PSA)和促卵泡激素(FSH)的评估。疗效分析基于选定的符合方案(PP)人群。
研究纳入的62例患者中,57例适合进行PP分析(37例HDE4;20例安慰剂)。24周时未发生与E4相关的严重心血管不良事件。HDE4组13.5%的患者报告每周出现HFs,安慰剂组为60.0%(P < 0.001)。每日出现HFs的比例分别为5.9%和55%。HDE4使骨转换参数显著降低(P < 0.0001)。总睾酮和游离睾酮下降更早(P < 0.05),游离睾酮进一步受到抑制(P < 0.05)。PSA抑制更显著且更早(P < 0.005)。FSH水平抑制率分别为98%和57%(P < 0.0001)。雌激素副作用为乳头敏感(34%)和男性乳房发育(17%)。
晚期前列腺癌ADT患者联合使用HDE4耐受性良好,24周时未观察到与治疗相关的心血管不良事件。HFs和骨转换显著减少。游离睾酮、PSA和FSH的抑制更快且更显著,表明联合使用HDE4可增强疾病控制。需要更大规模、更持久的研究来证实本研究报告的结果。
晚期前列腺癌患者雄激素剥夺疗法联合高剂量雌三醇治疗可减少潮热发生、保护骨骼并带来其他抗肿瘤益处。可能出现乳头敏感和男性乳房发育等副作用。