Department of Cardiology, Amsterdam UMC, Vrije Universiteit, ZH 5F003, De Boelelaan 1117, 1081 HV, Amsterdam, The Netherlands.
Department of Epidemiology and Biostatistics, Amsterdam UMC, Vrije Universiteit, Amsterdam, The Netherlands.
Int J Cardiovasc Imaging. 2021 Oct;37(10):3057-3068. doi: 10.1007/s10554-021-02355-4. Epub 2021 Aug 2.
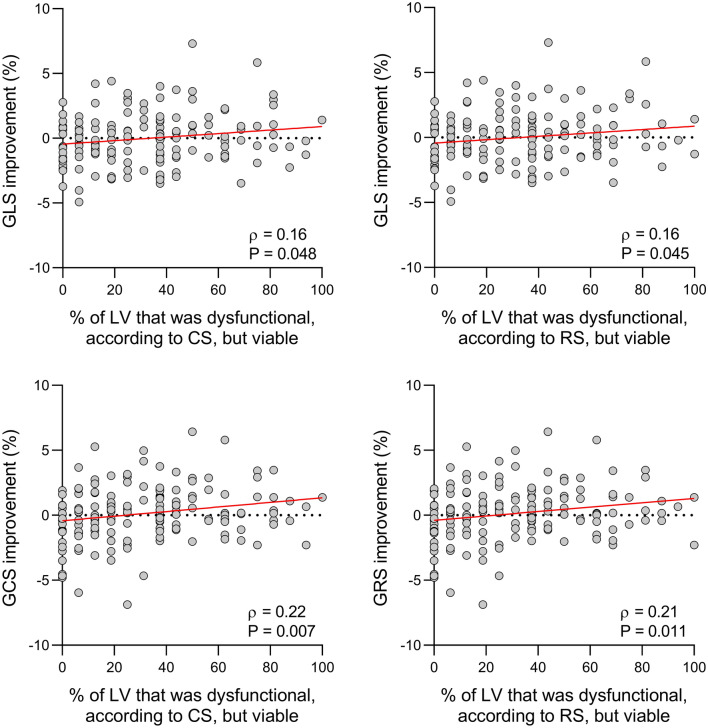
To evaluate the effect of percutaneous coronary intervention (PCI) of coronary chronic total occlusions (CTOs) on left ventricular (LV) strain assessed using cardiac magnetic resonance (CMR) tissue tracking. In 150 patients with a CTO, longitudinal (LS), radial (RS) and circumferential shortening (CS) were determined using CMR tissue tracking before and 3 months after successful PCI. In patients with impaired LV strain at baseline, global LS (10.9 ± 2.4% vs 11.6 ± 2.8%; P = 0.006), CS (11.3 ± 2.9% vs 12.0 ± 3.5%; P = 0.002) and RS (15.8 ± 4.9% vs 17.4 ± 6.6%; P = 0.001) improved after revascularization of the CTO, albeit to a small, clinically irrelevant, extent. Strain improvement was inversely related to the extent of scar, even after correcting for baseline strain (B = - 0.05; P = 0.008 for GLS, B = - 0.06; P = 0.016 for GCS, B = - 0.13; P = 0.017 for GRS). In the vascular territory of the CTO, dysfunctional segments showed minor improvement in both CS (10.8 [6.9 to 13.3] % vs 11.9 [8.1 to 15.0] %; P < 0.001) and RS (14.2 [8.4 to 18.7] % vs 16.0 [9.9 to 21.8] %; P < 0.001) after PCI. Percutaneous revascularization of CTOs does not lead to a clinically relevant improvement of LV function, even in the subgroup of patients and segments most likely to benefit from revascularization (i.e. LV dysfunction at baseline and no or limited myocardial scar).
评估经皮冠状动脉介入治疗(PCI)对冠状动脉慢性完全闭塞(CTO)患者左心室(LV)应变的影响,使用心脏磁共振(CMR)组织追踪技术进行评估。在 150 例 CTO 患者中,使用 CMR 组织追踪技术在成功 PCI 前和 3 个月后分别测量纵向(LS)、径向(RS)和周向缩短(CS)。在基线时 LV 应变受损的患者中,整体 LS(10.9±2.4% vs 11.6±2.8%;P=0.006)、CS(11.3±2.9% vs 12.0±3.5%;P=0.002)和 RS(15.8±4.9% vs 17.4±6.6%;P=0.001)在 CTO 血运重建后均有改善,但程度较小,无临床意义。应变改善与瘢痕程度呈负相关,即使在校正基线应变后(GLS 时 B= -0.05;P=0.008,GCS 时 B= -0.06;P=0.016,GRS 时 B= -0.13;P=0.017)。在 CTO 的血管区域,功能障碍节段 CS(10.8[6.9 至 13.3]% vs 11.9[8.1 至 15.0]%;P<0.001)和 RS(14.2[8.4 至 18.7]% vs 16.0[9.9 至 21.8]%;P<0.001)在 PCI 后也有轻微改善。即使在最有可能从血运重建中获益的患者和节段亚组(即基线时 LV 功能障碍和无或有限的心肌瘢痕)中,CTO 的经皮血运重建也不会导致 LV 功能的临床显著改善。