Tarragón Blanca, Ye Nan, Gallagher Martin, Sen Shaundeep, Portolés Jose Maria, Wang Amanda Y
Department of Nephrology, Hospital Universitario Puerta de Hierro Majadahonda, Madrid, Spain.
Renal and Metabolic Division, George Institute for Global Health, University of New South Wales, Sydney, NSW, Australia.
Clin Kidney J. 2020 Dec 12;14(8):1894-1900. doi: 10.1093/ckj/sfaa220. eCollection 2021 Aug.
Acute kidney injury (AKI) caused by cast nephropathy is associated with increased morbidity and mortality among patients with multiple myeloma (MM). High cut-off haemodialysis (HCO-HD) has proven to be effective in the removal of serum light chains but the effect on clinical outcomes, especially renal recovery, remains uncertain.
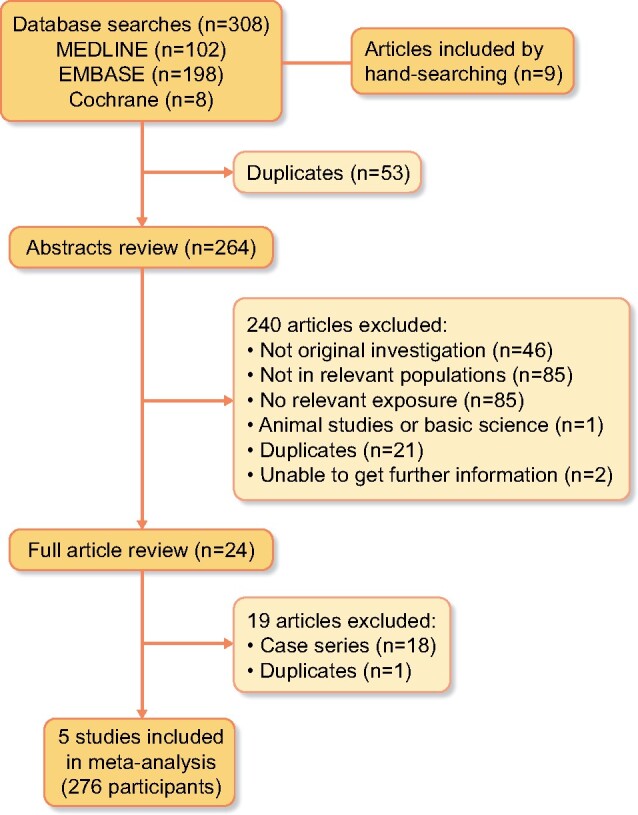
A systematic review and meta-analysis were performed examining all randomized controlled trials (RCTs) and observational studies (OBSs) assessing the effect of HCO-HD on clinical outcomes of patients with MM complicated by cast nephropathy-induced severe AKI. The primary outcome was all-cause mortality at the end of the study. The secondary outcomes included all-cause mortality at 12 months, HD independence and serum kappa and lambda light chain reduction. Pooled analysis was performed using random effects models.
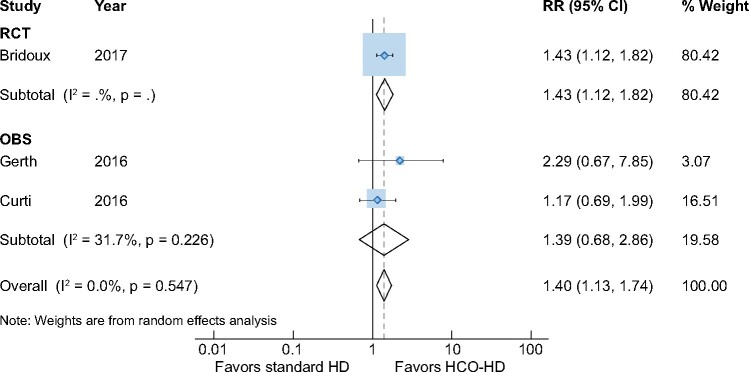
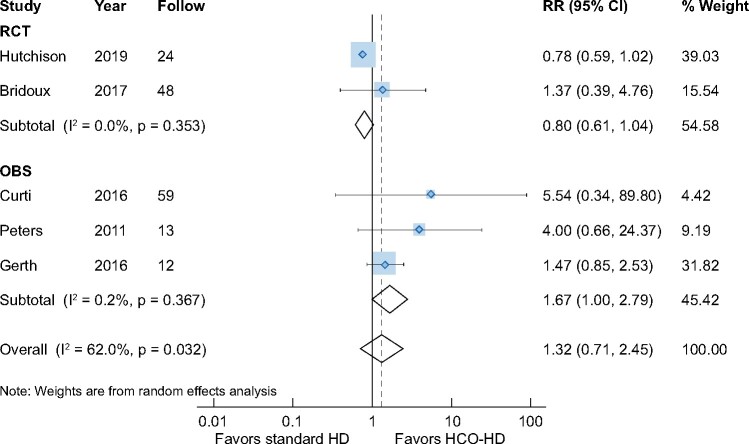
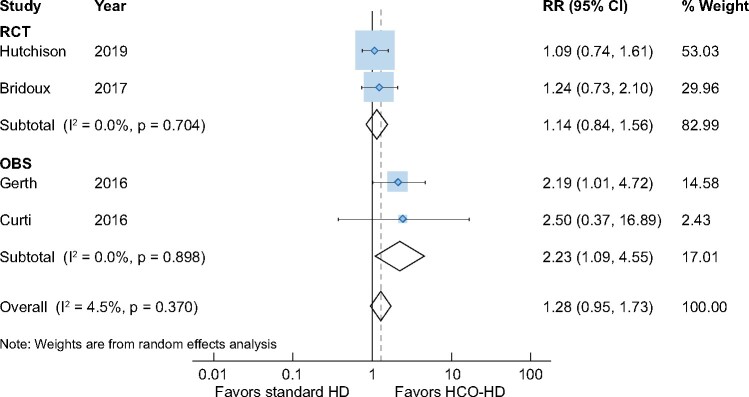
We identified five studies, comprising two RCTs and three retrospective cohort studies, including 276 patients with a mean follow-up of 18.7 months. The majority of the studies were of suboptimal quality and underpowered. Compared with patients treated with conventional HD, HCO-HD was not associated with a survival benefit at 12 months {five studies, 276 patients, relative risk [RR] 1.02 [95% confidence interval (CI) 0.76-1.35], = 33.9%} or at the end of the studies at an average of 34 months [five studies, 276 patients, RR 1.32 (95% CI 0.71-2.45), = 62.0%]. There was no difference in HD independence at 90 days [two trials, 78 patients, RR 2.23 (95% CI 1.09-4.55)], 6 months [two studies, 188 patients, RR 1.19 (95% CI 0.68-2.06)] or 12 months [two studies, 188 patients, RR 1.14 (95% CI 0.58-2.26)]. Patients receiving HCO dialysis, however, had a greater reduction in serum kappa [two studies, 188 patients, weighted mean difference (WMD) 46.7 (95% CI 38.6-54.7), = 52.0%] and lambda [two studies, 188 patients, WMD 50.3 (95% CI 21.4-79.3), = 95.1%] light chain levels.
Current evidence from RCTs and OBSs suggests HCO dialysis is able to reduce serum free light chains but makes no significant improvement in all-cause mortality and renal outcomes compared with conventional HD for patients with myeloma cast nephropathy. However, there is a trend towards better renal outcomes with the use of HCO dialysis. The lack of long-term data and the small sample sizes of the included studies limit this analysis. Therefore further large-scale RCTs with longer follow-up are needed to assess the effect of HCO dialysis on clinical outcomes in patients with myeloma cast nephropathy.
管型肾病所致急性肾损伤(AKI)与多发性骨髓瘤(MM)患者的发病率和死亡率增加相关。高截留血液透析(HCO-HD)已被证明在清除血清轻链方面有效,但对临床结局,尤其是肾脏恢复的影响仍不确定。
进行了一项系统评价和荟萃分析,纳入了所有评估HCO-HD对MM合并管型肾病所致严重AKI患者临床结局影响的随机对照试验(RCT)和观察性研究(OBS)。主要结局是研究结束时的全因死亡率。次要结局包括12个月时的全因死亡率、血液透析独立性以及血清κ和λ轻链降低情况。使用随机效应模型进行汇总分析。
我们纳入了五项研究,包括两项RCT和三项回顾性队列研究,共276例患者,平均随访18.7个月。大多数研究质量欠佳且效能不足。与接受常规血液透析的患者相比,HCO-HD在12个月时未显示出生存获益{五项研究,276例患者,相对危险度[RR] 1.02 [95%置信区间(CI)0.76 - 1.35],I² = 33.9%},在平均34个月的研究结束时也未显示出生存获益[五项研究,276例患者,RR 1.32(95% CI 0.71 - 2.45),I² = 62.0%]。在90天[两项试验,78例患者,RR 2.23(95% CI 1.09 - 4.55)]、6个月[两项研究,188例患者,RR 1.19(95% CI 0.68 - 2.06)]或12个月[两项研究,188例患者,RR 1.14(95% CI 0.58 - 2.26)]时,血液透析独立性方面无差异。然而,接受HCO血液透析的患者血清κ轻链[两项研究,188例患者,加权平均差(WMD)46.7(95% CI 38.6 - 54.7),I² = 52.0%]和λ轻链[两项研究,188例患者,WMD 50.3(95% CI 21.4 - 79.3),I² = 95.1%]水平下降幅度更大。
来自RCT和OBS的当前证据表明,对于骨髓瘤管型肾病患者,HCO血液透析能够降低血清游离轻链,但与常规血液透析相比,在全因死亡率和肾脏结局方面并无显著改善。然而,使用HCO血液透析有使肾脏结局更好的趋势。纳入研究缺乏长期数据且样本量小限制了本分析。因此,需要进一步开展大规模、随访时间更长的RCT来评估HCO血液透析对骨髓瘤管型肾病患者临床结局的影响。