Biliškov Ana Nevešćanin, Ivančev Božena, Pogorelić Zenon
Department of Anesthesiology, Reanimatology and Intensive Care, University Hospital of Split, Spinčićeva 1, 21000 Split, Croatia.
Department of Pediatric Surgery, University Hospital of Split, Spinčićeva 1, 21000 Split, Croatia.
Children (Basel). 2021 Jul 19;8(7):610. doi: 10.3390/children8070610.
Combining ketamine and propofol (ketofol) was suggested as a new concept for sedation and general anesthesia in pediatric populations for various conditions. The aim of the present study was to determine the effect of total intravenous anesthesia (TIVA) with propofol and ketofol on recovery after laparoscopic surgery in pediatric patients.
Two hundred children with median age of 5 years who underwent laparoscopic surgery were randomized into two groups. Propofol 1% was used for induction and maintenance of anesthesia in group I, while ketamine-propofol combination (ketofol) was used in group II. Ketamine-propofol combination (ketofol) was prepared in the same applicator for group II. Ketofol ratios of 1:4 and 1:7 were used for induction and maintenance of anesthesia, respectively. A reduced McFarlan infusion dose was used in group I (1.2, 1.0, and 0.8 mL/kg/h for 15, 15, and 30 min, respectively), while a McFarlan infusion dose was used in group II (1.5, 1.3, and 1.1 mL/kg/h for 15, 15, and 30 min, respectively). Extubating time, duration of anesthesia, and length of stay in post-anesthesia care unit (PACU) were recorded.
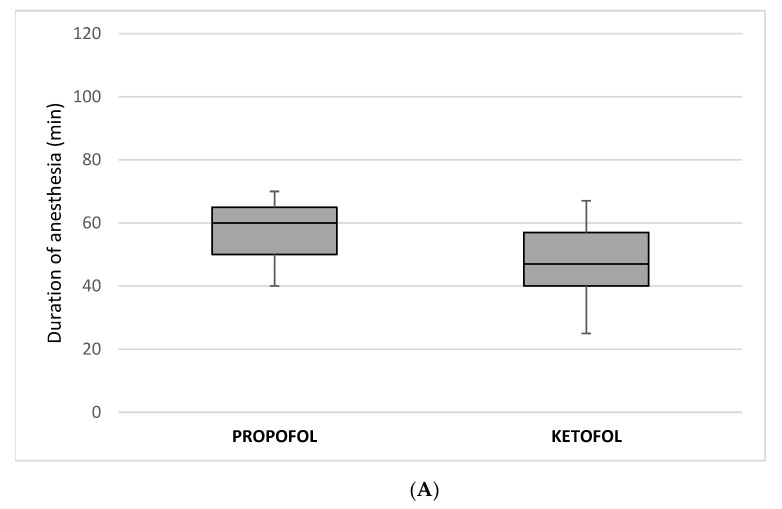
Extubating time was significantly lower in the ketofol group than in the propofol group (240 s vs. 530 s; < 0.00001). Significantly shorter duration of anesthesia (47 min vs. 60 min; < 0.00001) as well as length of stay in the PACU (35 min vs. 100 min; < 0.00001) were recorded in ketofol compared to the propofol group. Total fentanyl (100 µg (interquartile range, IQR 80, 125) vs. 50 µg (IQR 40, 60); < 0.00001) and propofol (260 mg (IQR 200, 350) vs. 160 mg (IQR 120, 210); < 0.00001) consumption per body weight were significantly lower in the ketofol group.
TIVA with ketamine-propofol combination (ketofol) using a reduced McFarlan dose regimen shortened extubating time, duration of anesthesia, as well as length of stay in the PACU in pediatric anesthesia after laparoscopic surgery.
氯胺酮与丙泊酚联合使用(氯胺酮-丙泊酚合剂)被认为是针对儿科多种情况进行镇静和全身麻醉的一种新概念。本研究的目的是确定丙泊酚和氯胺酮-丙泊酚合剂用于小儿患者腹腔镜手术后全静脉麻醉(TIVA)对恢复情况的影响。
200名中位年龄为5岁的接受腹腔镜手术的儿童被随机分为两组。第一组使用1%丙泊酚进行麻醉诱导和维持,而第二组使用氯胺酮-丙泊酚合剂。第二组的氯胺酮-丙泊酚合剂在同一注射器中配制。氯胺酮-丙泊酚合剂诱导和维持麻醉的比例分别为1:4和1:7。第一组使用降低的麦克法兰输注剂量(分别在15分钟、15分钟和30分钟时为1.2、1.0和0.8 mL/kg/h),而第二组使用麦克法兰输注剂量(分别在15分钟、15分钟和30分钟时为1.5、1.3和1.1 mL/kg/h)。记录拔管时间、麻醉持续时间以及在麻醉后护理单元(PACU)的停留时间。
氯胺酮-丙泊酚合剂组的拔管时间显著低于丙泊酚组(240秒对530秒;P<0.00001)。与丙泊酚组相比,氯胺酮-丙泊酚合剂组的麻醉持续时间显著缩短(47分钟对60分钟;P<0.00001),在PACU的停留时间也显著缩短(35分钟对100分钟;P<0.00001)。氯胺酮-丙泊酚合剂组每体重的芬太尼总量(100μg(四分位间距,IQR 80, 125)对50μg(IQR 40, 60);P<0.00001)和丙泊酚用量(260mg(IQR 200, 350)对160mg(IQR 120, 210);P<0.00001)显著更低。
采用降低的麦克法兰剂量方案的氯胺酮-丙泊酚合剂用于小儿腹腔镜手术后麻醉,可缩短拔管时间、麻醉持续时间以及在PACU的停留时间。