Zarębska-Michaluk Dorota, Jaroszewicz Jerzy, Parfieniuk-Kowerda Anna, Janczewska Ewa, Dybowska Dorota, Pawłowska Małgorzata, Halota Waldemar, Mazur Włodzimierz, Lorenc Beata, Janocha-Litwin Justyna, Simon Krzysztof, Piekarska Anna, Berak Hanna, Klapaczyński Jakub, Stępień Piotr, Sobala-Szczygieł Barbara, Citko Jolanta, Socha Łukasz, Tudrujek-Zdunek Magdalena, Tomasiewicz Krzysztof, Sitko Marek, Dobracka Beata, Krygier Rafał, Białkowska-Warzecha Jolanta, Laurans Łukasz, Flisiak Robert
Department of Infectious Diseases, Jan Kochanowski University, 25-317 Kielce, Poland.
Department of Infectious Diseases and Hepatology, Medical University of Silesia, 40-055 Katowice, Poland.
J Clin Med. 2021 Jul 25;10(15):3280. doi: 10.3390/jcm10153280.
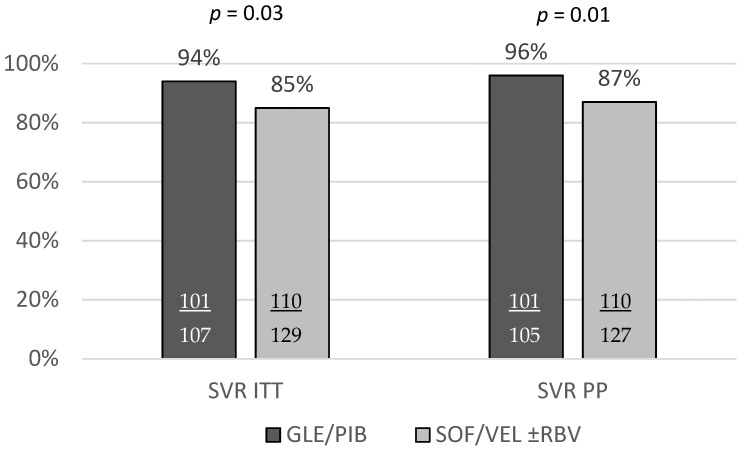
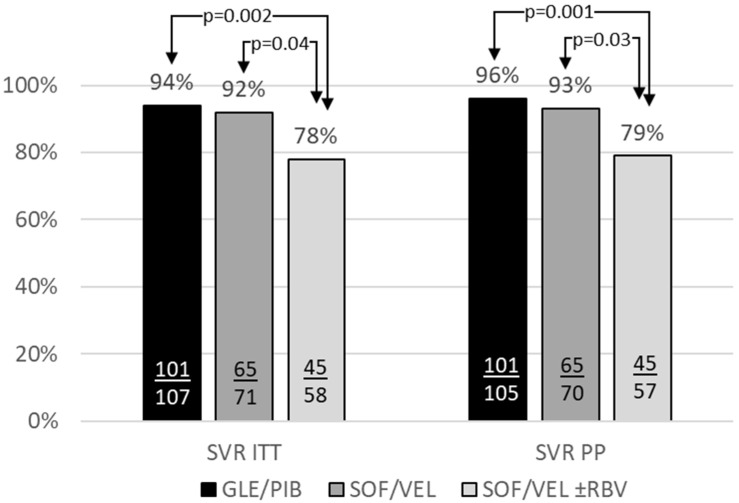
There is still limited data available from real-world experience studies on the pangenotypic regimens in patients with genotype (GT) 3 hepatitis C virus (HCV) infection and liver cirrhosis. The current study aimed to evaluate the efficacy and safety of pangenotypic regimens in this difficult-to-treat population. A total of 236 patients with mean age 52.3 ± 11.3 years and male predominance (72%) selected from EpiTer-2 database were included in the analysis; 72% of them were treatment-naïve. The majority of patients (55%) received the combination of sofosbuvir/velpatasvir (SOF/VEL), 71 without and 58 with ribavirin (RBV), whereas the remaining 107 individuals were assigned to glecaprevir/pibrentasvir (GLE/PIB). The effectiveness of the treatment following GLE/PIB and SOF/VEL regimens (96% and 93%) was higher compared to SOF/VEL + RBV option (79%). The univariate analysis demonstrated the significantly lower sustained virologic response in males, in patients with baseline HCV RNA ≥ 1,000,000 IU/mL, and among those who failed previous DAA-based therapy. The multivariate logistic regression analysis recognized only the male gender and presence of ascites at baseline as the independent factors of non-response to treatment. It should be emphasized that despite the availability of pangenotypic, strong therapeutic options, GT3 infected patients with cirrhosis still remain difficult-to-treat, especially those with hepatic impairment and DAA-experienced.
关于基因型(GT)3丙型肝炎病毒(HCV)感染合并肝硬化患者使用泛基因型治疗方案的真实世界经验研究数据仍然有限。本研究旨在评估泛基因型治疗方案在这一难治性人群中的疗效和安全性。从EpiTer - 2数据库中选取了236例平均年龄为52.3±11.3岁且男性占主导(72%)的患者纳入分析;其中72%为初治患者。大多数患者(55%)接受了索磷布韦/维帕他韦(SOF/VEL)联合治疗,71例未联用利巴韦林(RBV),58例联用了RBV,其余107例患者接受了格卡瑞韦/哌仑他韦(GLE/PIB)治疗。与SOF/VEL + RBV方案(79%)相比,GLE/PIB和SOF/VEL方案治疗后的有效率更高(分别为96%和93%)。单因素分析表明,男性、基线HCV RNA≥1,000,000 IU/mL的患者以及既往基于直接抗病毒药物(DAA)治疗失败的患者持续病毒学应答显著降低。多因素逻辑回归分析仅将男性性别和基线时存在腹水识别为治疗无应答的独立因素。应当强调的是,尽管有泛基因型的强效治疗方案,但GT3感染合并肝硬化的患者仍然难治,尤其是那些有肝功能损害和有DAA治疗史的患者。