Department of Population Science and Gene Health, National Heart and Lung Institute, Imperial College London, London, UK.
School of Cardiovascular Medicine & Sciences, King's College London British Heart Foundation Centre for Research Excellence, 125 Coldharbour Lane, London, SE5 9NU, UK.
BMC Med. 2021 Aug 10;19(1):179. doi: 10.1186/s12916-021-02048-8.
Patients with atrial fibrillation (AF) complicated by heart failure (HF) have a poor prognosis. We investigated whether long term loop-diuretic therapy in patients with AF and no known diagnosis of HF, as a potential surrogate marker of undiagnosed HF, is also associated with worse outcomes.
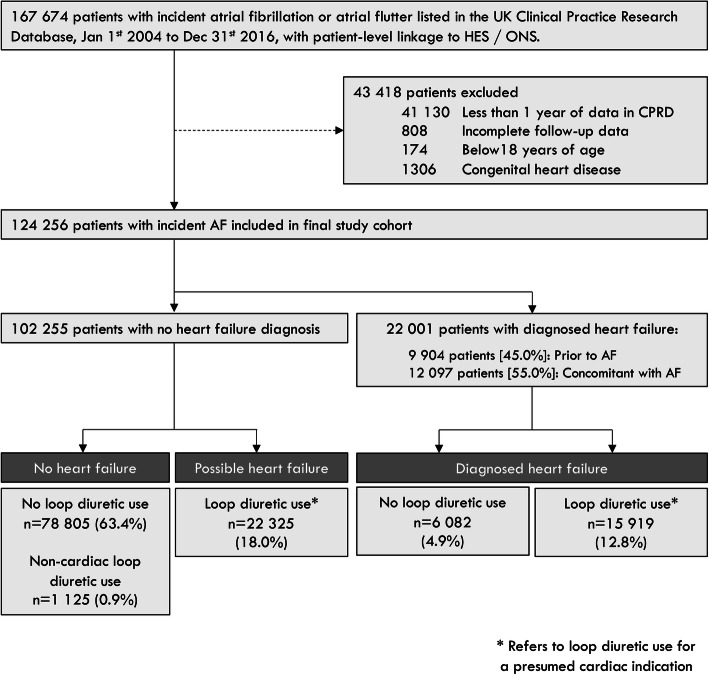
Adults with incident AF were identified from UK primary and secondary care records between 2004 and 2016. Repeat prescriptions for loop diuretics, without a diagnosis of HF or documented non-cardiac indication, were classified as 'isolated' loop diuretic use.
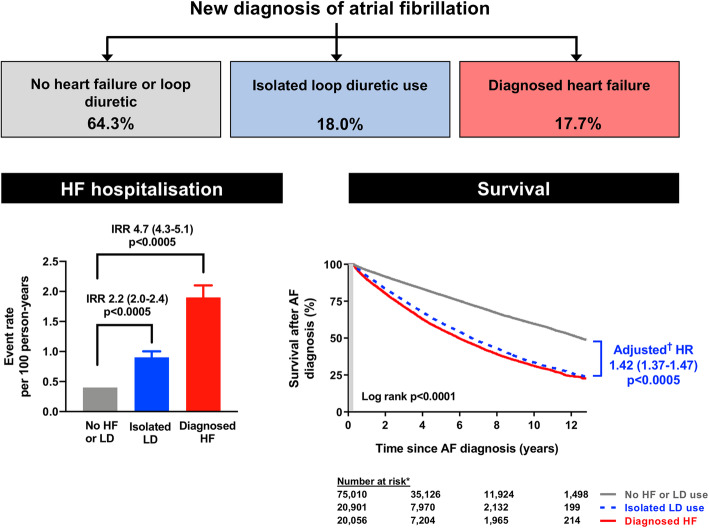
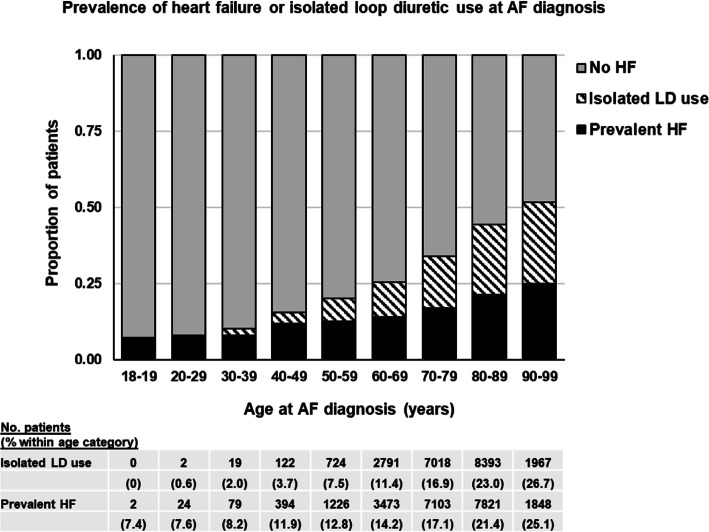
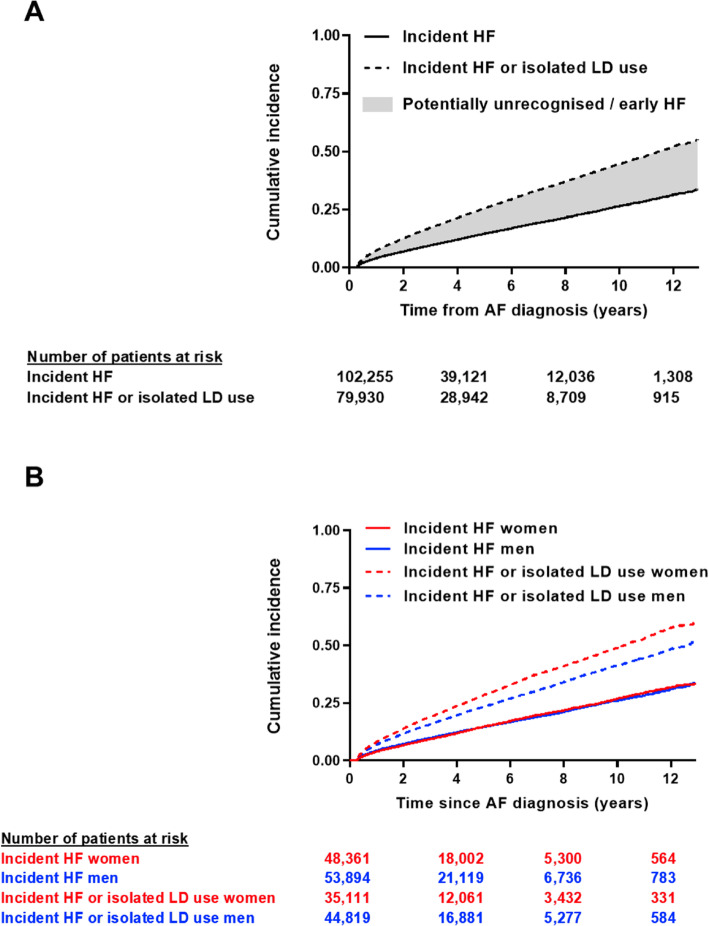
Amongst 124,256 people with incident AF (median 76 years, 47% women), 22,001 (17.7%) had a diagnosis of HF, and 22,325 (18.0%) had isolated loop diuretic use. During 2.9 (LQ-UQ 1-6) years' follow-up, 12,182 patients were diagnosed with HF (incidence rate 3.2 [95% CI 3.1-3.3]/100 person-years). Of these, 3999 (32.8%) had prior isolated loop diuretic use, including 31% of patients diagnosed with HF following an emergency hospitalisation. The median time from AF to HF diagnosis was 3.6 (1.2-7.7) years in men versus 5.1 (1.8-9.9) years in women (p = 0.0001). In adjusted models, patients with isolated loop diuretic use had higher mortality (HR 1.42 [95% CI 1.37-1.47], p < 0.0005) and risk of HF hospitalisation (HR 1.60 [95% CI 1.42-1.80], p < 0.0005) than patients with no HF or loop diuretic use, and comparably poor survival to patients with diagnosed HF.
Loop diuretics are commonly prescribed to patients with AF and may indicate increased cardiovascular risk. Targeted evaluation of these patients may allow earlier HF diagnosis, timely intervention, and better outcomes, particularly amongst women with AF, in whom HF appears to be under-recognised and diagnosed later than in men.
患有心房颤动(AF)合并心力衰竭(HF)的患者预后较差。我们研究了 AF 患者是否长期使用袢利尿剂治疗,因为这可能是未诊断 HF 的替代标志物,是否也与预后不良有关。
2004 年至 2016 年期间,我们从英国初级和二级保健记录中确定了患有新发 AF 的成年人。没有 HF 诊断或记录有非心脏适应证的重复处方袢利尿剂被归类为“孤立性”袢利尿剂使用。
在 124256 名患有新发 AF 的患者中(中位数 76 岁,47%为女性),22001 名(17.7%)有 HF 诊断,22325 名(18.0%)有孤立性袢利尿剂使用。在 2.9(LQ-UQ 1-6)年的随访期间,12182 名患者被诊断为 HF(发生率为 3.2[95%CI 3.1-3.3]/100 人年)。其中,3999 名(32.8%)有既往孤立性袢利尿剂使用史,包括 31%的 HF 诊断患者是在紧急住院后出现的。在男性中,从 AF 到 HF 诊断的中位时间为 3.6(1.2-7.7)年,而在女性中为 5.1(1.8-9.9)年(p = 0.0001)。在调整后的模型中,与没有 HF 或使用袢利尿剂的患者相比,使用孤立性袢利尿剂的患者死亡率更高(HR 1.42[95%CI 1.37-1.47],p<0.0005),HF 住院风险更高(HR 1.60[95%CI 1.42-1.80],p<0.0005),与诊断为 HF 的患者相比,生存情况也较差。
袢利尿剂通常用于 AF 患者,可能表明心血管风险增加。对这些患者进行有针对性的评估可能有助于更早地诊断 HF,及时进行干预,并改善预后,特别是在 AF 女性患者中,HF 的诊断似乎较晚,且比男性患者更晚。