Dohrn Maike F, Ellrichmann Gisa, Pjontek Rastislav, Lukas Carsten, Panse Jens, Gold Ralf, Schulz Jörg B, Gess Burkhard, Tauber Simone C
Department of Neurology, Medical Faculty of the RWTH Aachen University, Pauwelsstr. 30, Aachen, 52074, Germany.
Department of Neurology, St. Josef-Hospital, Ruhr-University Bochum, Bochum, Germany.
Ther Adv Neurol Disord. 2021 Jul 31;14:17562864211035543. doi: 10.1177/17562864211035543. eCollection 2021.
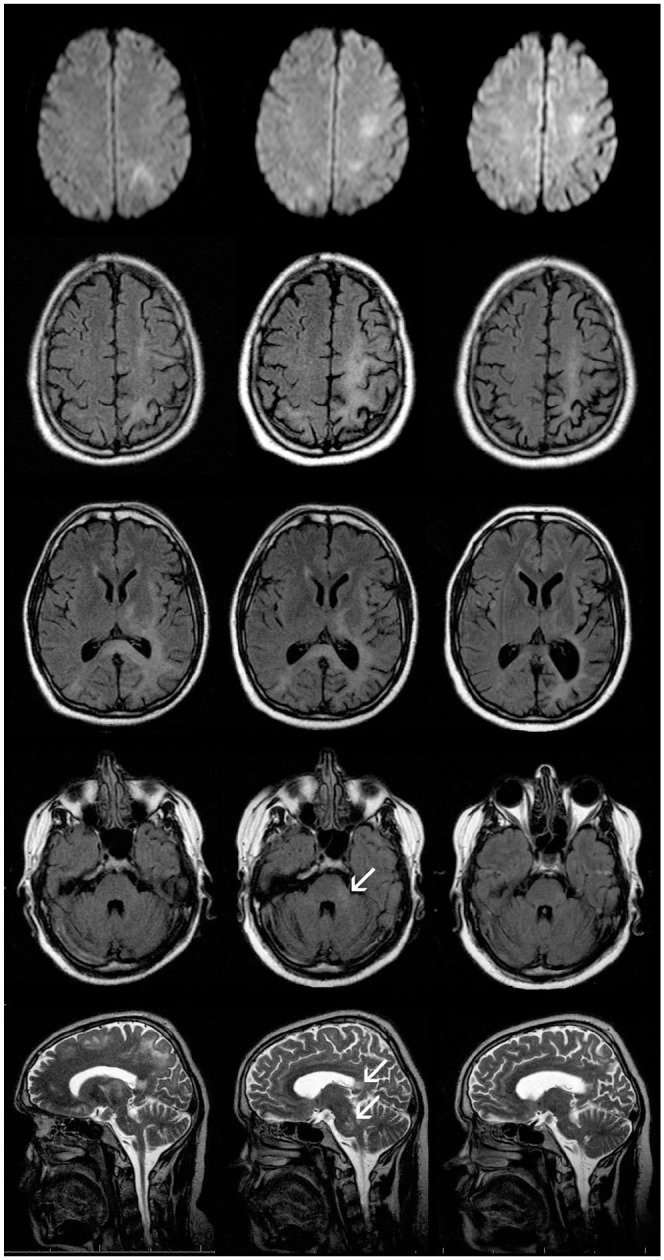
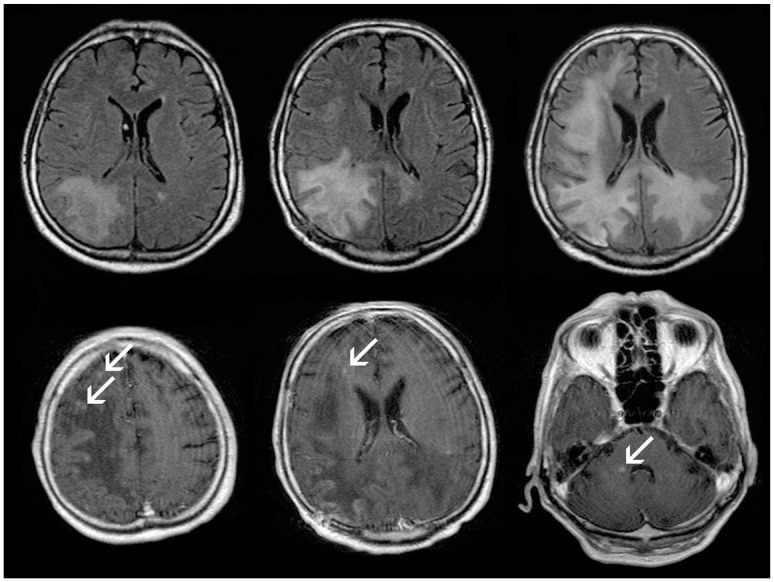
Progressive multifocal leukoencephalopathy (PML) is a subacute brain infection by the opportunistic John Cunningham (JC) virus. Herein, we describe seven patients with PML, lymphopenia, and sarcoidosis, in three of whom PML was the first manifestation of sarcoidosis. At onset, the clinical picture comprised rapidly progressive spastic hemi- or limb pareses as well as disturbances of vision, speech, and orientation. Cerebral magnetic resonance imaging showed T2-hyperintense, confluent, mainly supratentorial lesions. Four patients developed punctate contrast enhancement as a radiological sign of an immune reconstitution inflammatory syndrome (IRIS), three of them having a fatal course. In the cerebrospinal fluid, the initial JC virus load (8-25,787 copies/ml) did not correlate with interindividual severity; however, virus load corresponded to clinical dynamics. Brain biopsies ( = 2), performed 2 months after symptom onset, showed spotted demyelination and microglial activation. All patients had lymphopenia in the range of 270-1150/µl. To control JC virus, three patients received a combination of mirtazapine and mefloquine, another two patients additionally took cidofovir. One patient was treated with cidofovir only, and one patient had a combined regimen with mirtazapine, mefloquine, cidofovir, intravenous interleukin 2, and JC capsid vaccination. To treat sarcoidosis, the four previously untreated patients received prednisolone. Three patients had taken immunosuppressants prior to PML onset, which were subsequently stopped as a potential accelerator of opportunistic infections. After 6-54 months of follow up, three patients reached an incomplete recovery, one patient progressed, but survived so far, and two patients died. One further patient was additionally diagnosed with lung cancer, which he died from after 24 months. We conclude that the combination of PML and sarcoidosis is a diagnostic and therapeutic challenge. PML can occur as the first sign of sarcoidosis without preceding immunosuppressive treatment. The development of IRIS might be an indicator of poor outcome.
进行性多灶性白质脑病(PML)是由机会性感染的约翰·坎宁安(JC)病毒引起的亚急性脑部感染。在此,我们描述了7例患有PML、淋巴细胞减少症和结节病的患者,其中3例PML是结节病的首发表现。发病时,临床表现包括快速进展的痉挛性偏瘫或肢体轻瘫以及视力、言语和定向障碍。脑磁共振成像显示T2高信号、融合性、主要位于幕上的病变。4例患者出现点状对比增强,作为免疫重建炎症综合征(IRIS)的影像学表现,其中3例病情发展为致命性。脑脊液中,初始JC病毒载量(8 - 25,787拷贝/毫升)与个体间严重程度无关;然而,病毒载量与临床动态变化相符。症状出现2个月后进行的脑活检(n = 2)显示有散在性脱髓鞘和小胶质细胞活化。所有患者的淋巴细胞减少症程度在270 - 1150/微升之间。为控制JC病毒,3例患者接受了米氮平和甲氟喹的联合治疗,另外2例患者还加用了西多福韦。1例患者仅接受西多福韦治疗,1例患者采用了米氮平、甲氟喹、西多福韦、静脉注射白细胞介素2和JC衣壳疫苗的联合治疗方案。为治疗结节病,4例先前未接受治疗的患者接受了泼尼松龙治疗。3例患者在PML发病前服用过免疫抑制剂,随后作为机会性感染的潜在促进因素而停药。经过6 - 54个月的随访,3例患者达到不完全康复,1例患者病情进展,但至今存活,2例患者死亡。另有1例患者被额外诊断出患有肺癌,24个月后死于肺癌。我们得出结论,PML和结节病的合并存在是一个诊断和治疗上的挑战。PML可能作为结节病的首发症状出现,且无前驱免疫抑制治疗史。IRIS的发生可能是预后不良的一个指标。