Maleki Arash, Look-Why Sydney, Manhapra Ambika, Foster C Stephen
Massachusetts Eye Research and Surgery Institution, Waltham, MA, United States.
The Ocular Immunology and Uveitis Foundation, Waltham, MA, United States.
J Ophthalmic Vis Res. 2021 Jul 29;16(3):490-501. doi: 10.18502/jovr.v16i3.9443. eCollection 2021 Jul-Sep.
To report two cases; bilateral arteritic anterior ischemic optic neuropathy (AAION) and bilateral acute zonal occult outer retinopathy (AZOOR) after COVID-19 mRNA vaccination.
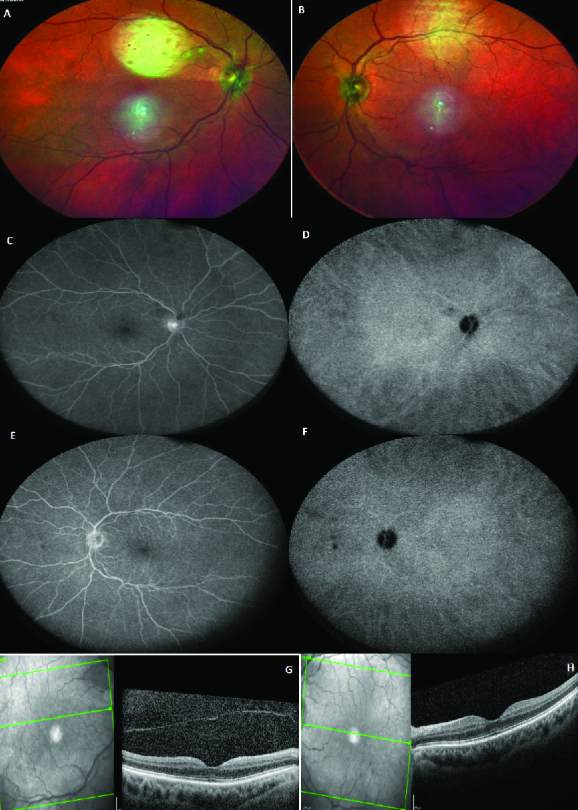
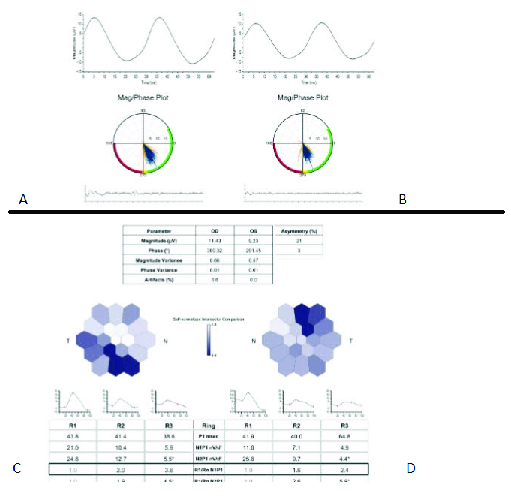
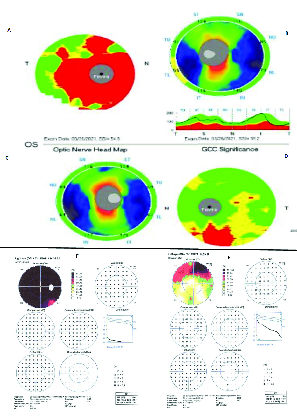
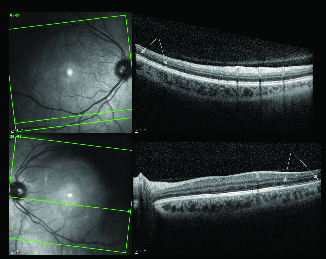
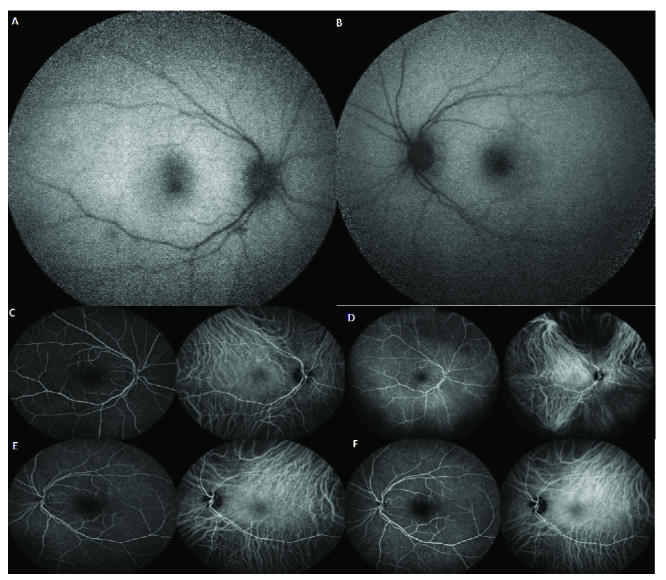
The first patient was a 79-year-old female was presented to us 35 days after a sudden bilateral loss of vision, which occurred two days after receiving the second recombinant mRNA vaccine (Pfizer) injection. Temporal artery biopsy was compatible with AAION. At presentation, the best-corrected visual acuity was 20/1250 and 20/40 in the right and left eyes on the Snellen acuity chart, respectively. There was 3+ afferent pupillary defect in the right eye. The anterior segment and posterior segment exams were normal except for pallor of the optic nerve head in both eyes. Intraocular pressure was normal in both eyes. She was diagnosed with bilateral AAION and Subcutaneous tocilizumab 162 mg weekly was recommended with monitoring her ESR, CRP, and IL-6.The second patient was a 33-year-old healthy female who was referred to us for a progressive nasal field defect in her left eye, and for flashes in both eyes. Her symptoms started 10 days after receiving the second recombinant mRNA vaccine (Moderna) injection. Complete bloodwork performed by a uveitis specialist demonstrated high ESR (25) and CRP (19) levels. As a result, she was diagnosed with unilateral AZOOR in her left eye and was subsequently treated with an intravitreal dexamethasone implant in the same eye. At presentation, vision was20/20 in both eyes. The anterior segment and posterior segment exams were completely normal except for the presence of abnormal white reflex in the temporal macula of her left eye. We diagnosed her with bilateral AZOOR. Since she was nursing, intravitreal dexamethasone implant was recommended for the right eye.
There may be a correlation between ocular inflammatory diseases with autoimmune mechanism and the mRNA COVID-19 vaccination.
报告两例新型冠状病毒病(COVID-19)信使核糖核酸(mRNA)疫苗接种后发生的双侧动脉炎性前部缺血性视神经病变(AAION)和双侧急性区域性隐匿性外层视网膜病变(AZOOR)病例。
首例患者为一名79岁女性,在接受第二剂重组mRNA疫苗(辉瑞)注射两天后突然出现双眼视力丧失,35天后前来就诊。颞动脉活检结果符合AAION。就诊时,在斯内伦视力表上,右眼最佳矫正视力为20/1250,左眼为20/40。右眼有3+传入性瞳孔障碍。除双眼视神经乳头苍白外,眼前节和后节检查均正常。双眼眼压正常。她被诊断为双侧AAION,建议每周皮下注射托珠单抗162毫克,并监测其红细胞沉降率(ESR)、C反应蛋白(CRP)和白细胞介素-6(IL-6)。第二例患者是一名33岁的健康女性,因左眼进行性鼻侧视野缺损和双眼闪光前来就诊。她的症状在接受第二剂重组mRNA疫苗(莫德纳)注射10天后开始出现。葡萄膜炎专科医生进行的全血细胞检查显示ESR(25)和CRP(19)水平升高。因此,她被诊断为左眼单侧AZOOR,随后在同一只眼内植入了地塞米松玻璃体内植入物。就诊时,双眼视力均为正常。除左眼颞侧黄斑区存在异常白色反光外,眼前节和后节检查完全正常。我们诊断她为双侧AZOOR。由于她正在哺乳期,建议右眼植入地塞米松玻璃体内植入物。
自身免疫机制的眼部炎性疾病与COVID-19 mRNA疫苗接种之间可能存在关联。