Hematology Department, Hospital 12 de Octubre i+12, CNIO, Complutense University, Madrid, Spain.
Department of Medicine, Division of Hematology-Oncology, University of California San Francisco, San Francisco, USA.
J Hematol Oncol. 2021 Aug 17;14(1):126. doi: 10.1186/s13045-021-01135-w.
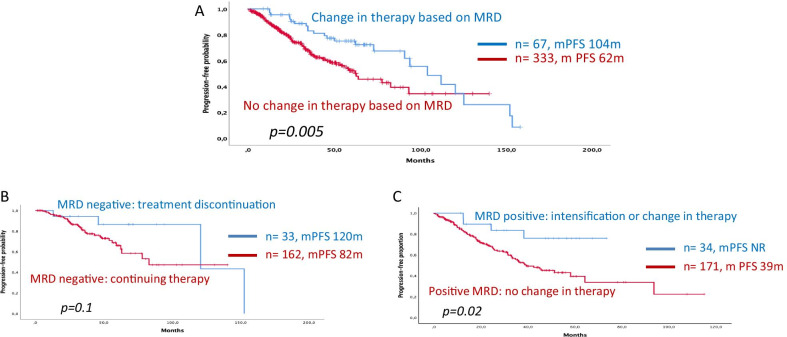
The assessment of measurable residual disease (MRD) in bone marrow has proven of prognostic relevance in patients with multiple myeloma (MM). Nevertheless, and unlike other hematologic malignancies, the use of MRD results to make clinical decisions in MM has been underexplored to date. In this retrospective study, we present the results from a multinational and multicenter series of 400 patients with MRD monitoring during front-line therapy with the aim of exploring how clinical decisions made based on those MRD results affected outcomes. As expected, achievement of MRD negativity at any point was associated with improved PFS versus persistent MRD positivity (median PFS 104 vs. 45 months, p < 0.0001). In addition, however, 67 out of 400 patients underwent a clinical decision (treatment discontinuation, intensification or initiation of a new therapy) based on MRD results. Those patients in whom a treatment change was made showed a prolonged PFS in comparison with those 333 patients in which MRD results were not acted upon (respectively, mPFS 104 vs. 62 months, p = 0.005). In patients who achieved MRD negativity during maintenance (n = 186) on at least one occasion, stopping therapy in 24 patients vs. continuing in 162 did not alter PFS (mPFS 120 months vs. 82 months, p = 0.1). Most importantly, however, in patients with a positive MRD during maintenance (n = 214), a clinical decision (either intensification or change of therapy) (n = 43) resulted in better PFS compared to patients in whom no adjustment was made (n = 171) (mPFS NA vs. 39 months, p = 0.02). Interestingly, there were no significant differences when MRD was assessed by flow cytometry or by next-generation sequencing. Herein, we find that MRD is useful in guiding clinical decisions during initial therapy and has a positive impact on PFS in MM patients. This potentially opens a new dimension for the use of MRD in MM, but this role still remains to be confirmed in prospective, randomized clinical trials.
骨髓中可测量残留疾病(MRD)的评估已被证明与多发性骨髓瘤(MM)患者的预后相关。然而,与其他血液恶性肿瘤不同,迄今为止,MRD 结果在 MM 中的临床决策中的应用尚未得到充分探索。在这项回顾性研究中,我们展示了一项针对 400 例患者的多国家和多中心系列研究的结果,这些患者在一线治疗期间进行了 MRD 监测,旨在探讨基于这些 MRD 结果做出的临床决策如何影响结局。正如预期的那样,任何时间点达到 MRD 阴性均与持续 MRD 阳性相比具有更好的 PFS(中位 PFS 104 与 45 个月,p<0.0001)。此外,然而,400 例患者中有 67 例根据 MRD 结果做出了临床决策(停止治疗、强化或开始新的治疗)。与未进行 MRD 结果处理的 333 例患者相比,进行治疗改变的患者具有更长的 PFS(分别为 mPFS 104 与 62 个月,p=0.005)。在至少一次维持治疗期间达到 MRD 阴性的 186 例患者中,24 例患者停止治疗与 162 例患者继续治疗并未改变 PFS(mPFS 120 与 82 个月,p=0.1)。然而,最重要的是,在维持治疗期间 MRD 阳性的 214 例患者中,临床决策(强化或改变治疗)(n=43)与未进行调整的患者(n=171)相比,具有更好的 PFS(mPFS 无数据与 39 个月,p=0.02)。有趣的是,通过流式细胞术或下一代测序评估 MRD 时没有差异。在此,我们发现 MRD 可用于指导初始治疗期间的临床决策,并对 MM 患者的 PFS 产生积极影响。这可能为 MM 中 MRD 的应用开辟了一个新的维度,但这一作用仍需在前瞻性、随机临床试验中得到证实。