Chen Shaozhen, Lin Kangni, Li Qian, Luo Xiaofeng, Xiao Min, Chen Minmin, Zhu Haojie, Chen Yongquan, Wu Xueqiong, Zeng Yanling, Zhang Yuxin, Ally Issa Hajji, Xu Jingjing, Ren Jinhua, Chen Zhizhe, Hu Jianda, Yang Ting
Fujian Institute of Hematology, Fujian Provincial Key Laboratory on Hematology, Fujian Medical University Union Hospital, Fuzhou 350001, Fujian, P. R. China.
Department of Cancer, Fujian Provincial Cancer Hospital, Fuzhou 350014, Fujian, P. R. China.
J Cancer. 2021 Jul 25;12(18):5494-5505. doi: 10.7150/jca.50802. eCollection 2021.
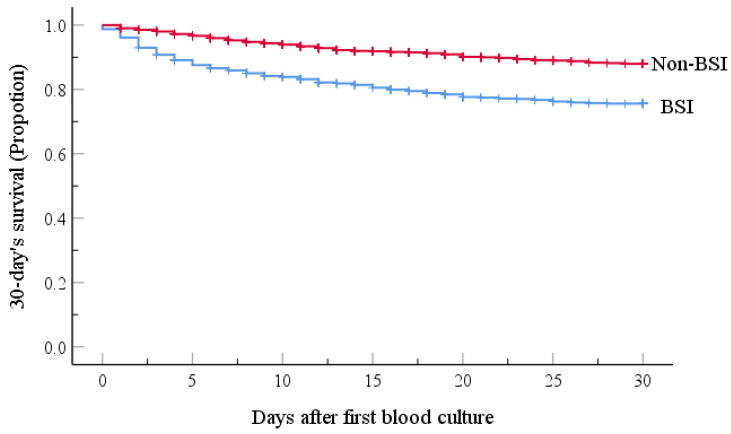
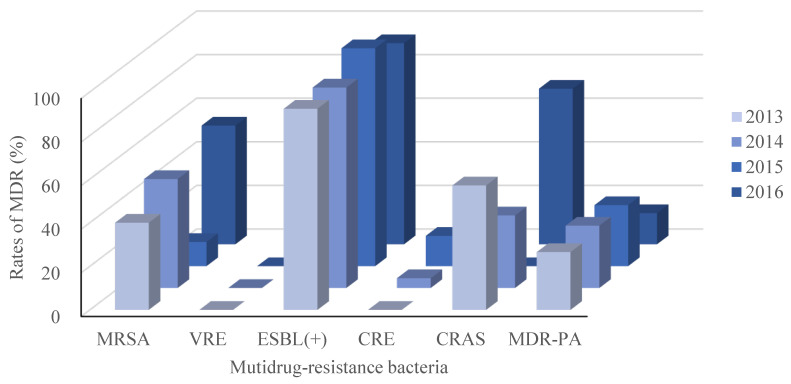
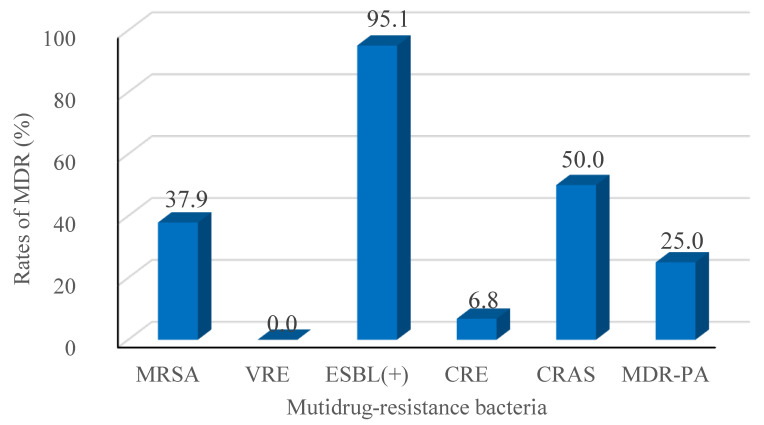
Bloodstream infection (BSI) is a common and serious complication after patients with hematologic malignancies (HM) receiving chemotherapy. This study examined real-world data seeking to characterize HM BSI and identify risk factors for BSI emergence and mortality. We retrospectively analyzed the pathogenic epidemiology, antibiotic resistance, and BSI risk factors in a single-center cohort including 3014 consecutive patients with HM receiving chemotherapy between 2013 and 2016. Results of the pathogenic epidemiology were validated via comparison to available reported data. We found that 725 patients (24.1%) had BSIs. Gram-negative (G-) bacteria represented 64.7% of the 744 isolated pathogenic strains, while Gram-positive (G+) bacteria and fungi accounted for 27.7% and 7.7% of the BSIs, respectively. The most common isolates were (19.2%), and 95.1% of the multidrug-resistant strains (MDR) were extended-spectrum beta-lactamase producing strains. G- bacteria were the main microflora responsible for BSI in our cohort of Chinese HM patients compared to studies in developed countries or in neutropenic children with HM or solid tumors. Multivariate analysis revealed that male sex, age ≥ 45 and < 65 yr, hospital length of stay ≥ 9d, neutropenia ≥ 7d before cultures, ≥ 2 antibiotics, and infections (gastrointestinal, perirectal, or urinary tract) independently predicted BSI emergence. Furthermore, age ≥ 65 yr, neutropenia ≥ 7d before blood cultures, no HM remission, lower white blood cell count, ≥ 3 antibiotics, respiratory infections, and and BSI were independent predictors of 30-day mortality. G- bacteria were the predominant microflora during the study period and antibiotic resistance levels of the pathogens detected were high, especially for MDR strains. The mortality of BSI patients was high in this large cohort. Close attention should be paid to the risk factors identified here to facilitate timely and effective clinical management of such patients.
血流感染(BSI)是血液系统恶性肿瘤(HM)患者接受化疗后常见且严重的并发症。本研究分析了真实世界数据,旨在描述HM患者BSI的特征,并确定BSI发生及死亡的危险因素。我们回顾性分析了2013年至2016年间在单中心队列中连续接受化疗的3014例HM患者的病原流行病学、抗生素耐药性及BSI危险因素。通过与现有报告数据比较来验证病原流行病学结果。我们发现725例患者(24.1%)发生了BSI。在744株分离出的致病菌株中,革兰氏阴性(G-)菌占64.7%,而革兰氏阳性(G+)菌和真菌分别占BSI的27.7%和7.7%。最常见的分离菌为 (19.2%),95.1%的多重耐药(MDR)菌株为产超广谱β-内酰胺酶菌株。与发达国家或患有HM或实体瘤的中性粒细胞减少儿童的研究相比,G-菌是我们中国HM患者队列中导致BSI的主要微生物群。多因素分析显示,男性、年龄≥45岁且<65岁、住院时间≥9天、培养前中性粒细胞减少≥7天、使用≥2种抗生素以及感染(胃肠道、直肠周围或泌尿系统)可独立预测BSI的发生。此外,年龄≥65岁、血培养前中性粒细胞减少≥7天、HM未缓解、白细胞计数较低、使用≥3种抗生素、呼吸道感染以及 及BSI是30天死亡率的独立预测因素。在研究期间,G-菌是主要的微生物群,检测到的病原体的抗生素耐药水平较高,尤其是MDR菌株。在这个大型队列中,BSI患者的死亡率较高。应密切关注此处确定的危险因素,以便对此类患者进行及时有效的临床管理。