Wilkie Joel R, Lipson Rachel, Johnson Matthew C, Williams Christina, Moghanaki Drew, Elliott David, Owen Dawn, Atluri Namratha, Jolly Shruti, Chapman Christina Hunter
Center for Clinical Management Research, Veterans Affairs Ann Arbor Healthcare System, Ann Arbor, Michigan.
Department of Radiation Oncology, University of Michigan, Ann Arbor, Michigan.
Adv Radiat Oncol. 2021 Apr 20;6(4):100707. doi: 10.1016/j.adro.2021.100707. eCollection 2021 Jul-Aug.
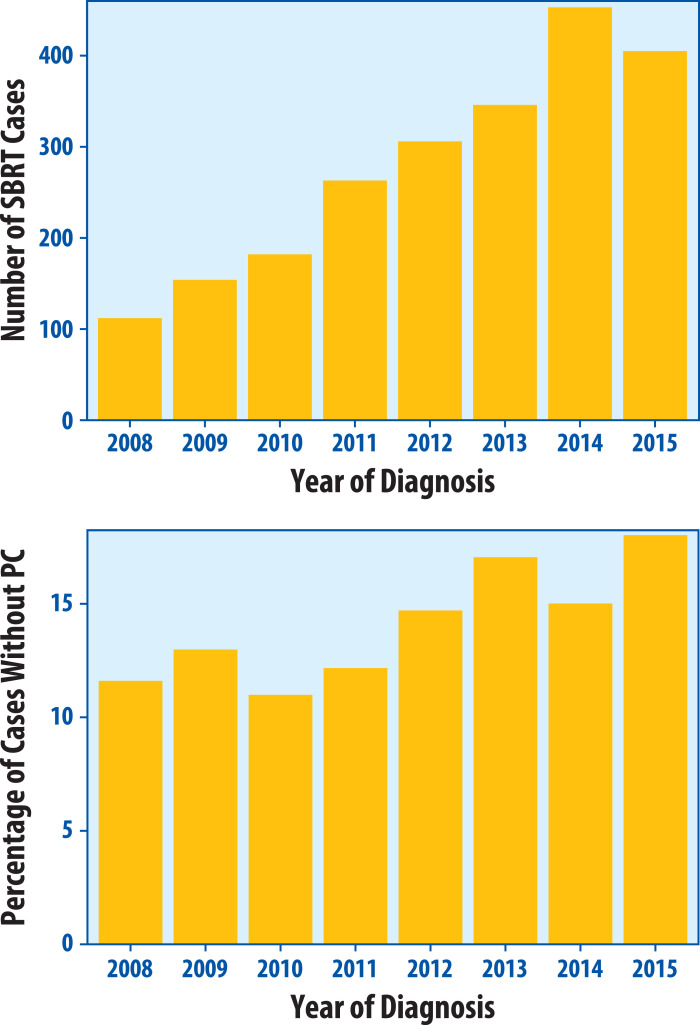
Stereotactic body radiation therapy (SBRT) use has increased among patients without pathologic confirmation (PC) of lung cancer. Empirical SBRT without PC raises concerns about variation in workup and patient selection, but national trends have not been well described. In this study, we assessed patterns of empirical SBRT use, workup, and causes of death among a large national non-small cell lung cancer (NSCLC) cohort.
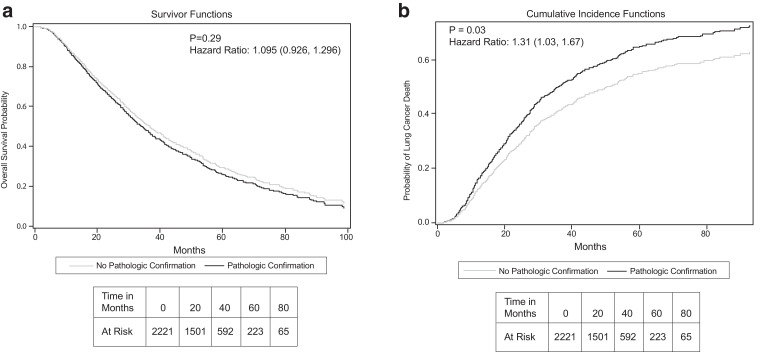
We identified 2221 patients treated with SBRT for cT1-T2aN0M0 NSCLC in the Veterans Affairs health care system from 2008 to 2015. We reviewed their pretreatment workup and assessed associations between absence of PC and clinical and demographic factors. We compared causes of death between PC and non-PC groups and used Cox proportional hazards modeling to compare overall survival and lung cancer specific survival (LCSS) between these groups.
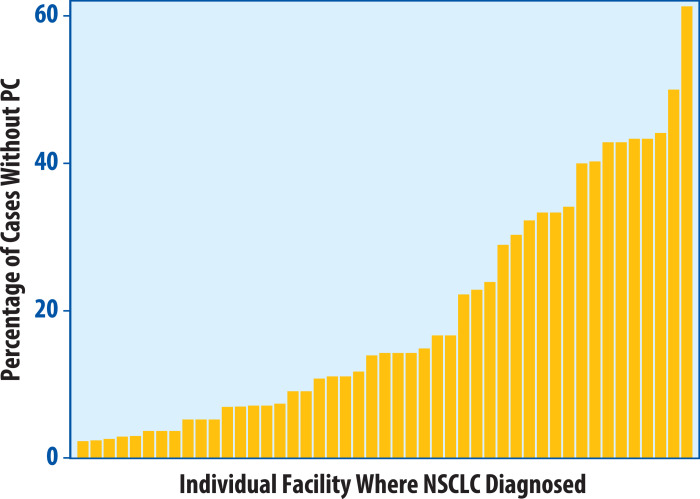
Treatment without PC varied from 0% to 61% among Veterans Affairs medical centers, with at least 5 cases of stage I NSCLC. Overall, 14.9% of patients were treated without PC and 8.8% did not have a biopsy attempt. Ten percent of facilities were responsible for almost two-thirds (62%) of cases of treatment without PC. Of non-PC patients, 95.5% had positron emission tomography scans, 40.6% had biopsy procedures attempted, and 12.7% underwent endobronchial ultrasound. Non-PC patients were more likely to have cT1 tumors and live outside the histoplasmosis belt. Age, sex, smoking status, and Charlson comorbidity index were similar between groups. Lung cancer was the most common cause of death in both groups. Overall survival was similar between groups, whereas non-PC patients had better LCSS (hazard ratio = 0.77, = .031).
Empirical SBRT use varied widely among institutions and appropriate radiographic workup was consistently used in this national cohort. Future studies should investigate determinants of variation and reasons for higher LCSS among non-PC patients.
在未获得肺癌病理确诊(PC)的患者中,立体定向体部放射治疗(SBRT)的使用有所增加。未经病理确诊的经验性SBRT引发了对检查流程和患者选择差异的担忧,但全国范围内的趋势尚未得到充分描述。在本研究中,我们评估了一个大型全国性非小细胞肺癌(NSCLC)队列中经验性SBRT的使用模式、检查流程及死亡原因。
我们在退伍军人事务医疗保健系统中确定了2008年至2015年期间接受SBRT治疗的cT1-T2aN0M0 NSCLC患者2221例。我们回顾了他们的治疗前检查流程,并评估了未进行病理确诊与临床及人口统计学因素之间的关联。我们比较了病理确诊组和未病理确诊组的死亡原因,并使用Cox比例风险模型比较了两组之间的总生存期和肺癌特异性生存期(LCSS)。
在退伍军人事务医疗中心中,未进行病理确诊的治疗比例从0%到61%不等,其中至少有5例I期NSCLC患者。总体而言,14.9%的患者在未进行病理确诊的情况下接受了治疗,8.8%的患者未尝试进行活检。几乎三分之二(62%)的未进行病理确诊治疗病例是由10%的机构负责的。在未进行病理确诊的患者中,95.5%进行了正电子发射断层扫描,40.6%尝试了活检程序,12.7%接受了支气管内超声检查。未进行病理确诊的患者更有可能患有cT1肿瘤,并且居住在组织胞浆菌病带以外。两组之间的年龄、性别、吸烟状况和Charlson合并症指数相似。肺癌是两组中最常见的死亡原因。两组之间的总生存期相似,而未进行病理确诊的患者具有更好的肺癌特异性生存期(风险比 = 0.77,P = 0.031)。
经验性SBRT的使用在各机构之间差异很大,并且在这个全国性队列中始终采用了适当的影像学检查流程。未来的研究应调查差异的决定因素以及未进行病理确诊的患者中肺癌特异性生存期较高的原因。