Cho Jin, Place Krystal, Salstrand Rebecca, Rahmat Monireh, Mansouri Misagh, Fell Nancy, Sartipi Mina
Department of Computer Science and Engineering, University of Tennessee at Chattanooga, USA.
Center for Urban Informatics and Progress, University of Tennessee at Chattanooga, USA.
Stroke Res Treat. 2021 Aug 19;2021:5546766. doi: 10.1155/2021/5546766. eCollection 2021.
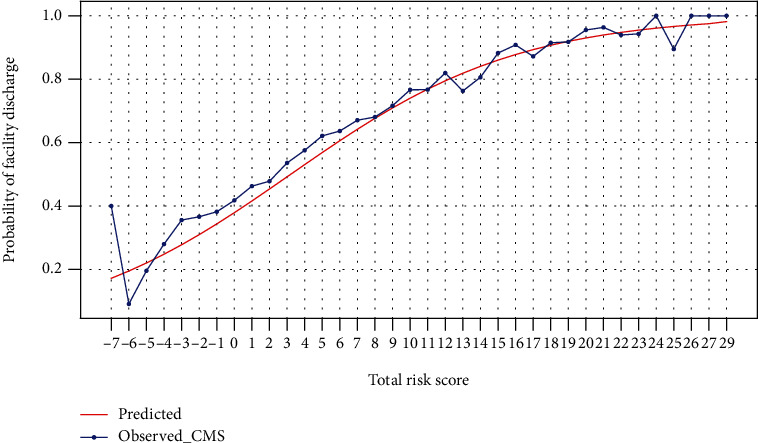
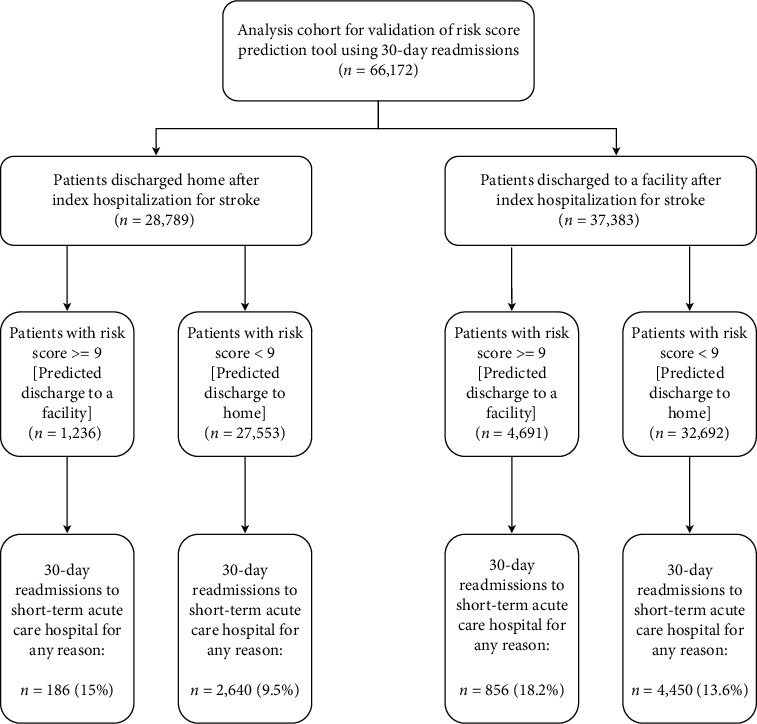
After short-term, acute-care hospitalization for stroke, patients may be discharged home or other facilities for continued medical or rehabilitative management. The site of postacute care affects overall mortality and functional outcomes. Determining discharge disposition is a complex decision by the healthcare team. Early prediction of discharge destination can optimize poststroke care and improve outcomes. Previous attempts to predict discharge disposition outcome after stroke have limited clinical validations. In this study, readmission status was used as a measure of the clinical significance and effectiveness of a discharge disposition prediction. Low readmission rates indicate proper and thorough care with appropriate discharge disposition. We used Medicare beneficiary data taken from a subset of base claims in the years of 2014 and 2015 in our analyses. A predictive tool was created to determine discharge disposition based on risk scores derived from the coefficients of multivariable logistic regression related to an adjusted odds ratio. The top five risk scores were admission from a skilled nursing facility, acute heart attack, intracerebral hemorrhage, admission from "other" source, and an age of 75 or older. Validation of the predictive tool was accomplished using the readmission rates. A 75% probability for facility discharge corresponded with a risk score of greater than 9. The prediction was then compared to actual discharge disposition. Each cohort was further analyzed to determine how many readmissions occurred in each group. Of the actual home discharges, 95.7% were predicted to be there. However, only 47.8% of predictions for home discharge were actually discharged home. Predicted discharge to facility had 15.9% match to the actual facility discharge. The scenario of actual discharge home and predicted discharge to facility showed that 186 patients were readmitted. Following the algorithm in this scenario would have recommended continued medical management of these patients, potentially preventing these readmissions.
中风患者在短期急性护理住院治疗后,可能会出院回家或转至其他机构接受持续的医疗或康复管理。急性后期护理的地点会影响总体死亡率和功能结局。确定出院处置是医疗团队做出的复杂决策。早期预测出院去向可优化中风后护理并改善结局。以往预测中风后出院处置结果的尝试临床验证有限。在本研究中,再入院状态被用作出院处置预测的临床意义和有效性的衡量指标。低再入院率表明护理得当且彻底,出院处置合适。我们在分析中使用了2014年和2015年从基础索赔子集获取的医疗保险受益人的数据。基于与调整后的优势比相关的多变量逻辑回归系数得出的风险评分,创建了一个预测工具来确定出院处置。前五个风险评分是来自熟练护理机构的入院、急性心脏病发作、脑出血、来自“其他”来源的入院以及年龄在75岁及以上。使用再入院率完成了预测工具的验证。机构出院概率为75%时对应的风险评分大于9。然后将该预测与实际出院处置进行比较。对每个队列进一步分析以确定每组发生了多少次再入院。在实际出院回家的患者中,95.7%被预测会出院回家。然而,预测出院回家的患者中只有47.8%实际出院回家。预测出院至机构的情况与实际机构出院的匹配率为15.9%。实际出院回家但预测出院至机构的情况显示有186名患者再次入院。按照此场景中的算法,本可建议对这些患者继续进行医疗管理,有可能防止这些再入院情况的发生。