Department of Internal Medicine, Chonnam National University Medical School, 160, Baekseo-ro, Dong-gu, 61469, Gwangju, South Korea.
Department of Pathology, Chonnam National University Medical School, 160, Baekseo-ro, Dong-gu, 61469, Gwangju, South Korea.
BMC Endocr Disord. 2021 Aug 30;21(1):177. doi: 10.1186/s12902-021-00839-x.
Thyroid stimulating hormone (TSH) secreting pituitary adenoma (TSHoma) with coexisting thyroid cancer is extremely rare, and proper treatment of both diseases may pose a unique clinical challenge. When TSHoma has plurihormonality, particularly involving the co-secretion of growth hormone (GH), management can be more complicated. Herein, we present a difficult-to-manage case of papillary thyroid cancer with an incurable TSH/GH-secreting pituitary adenoma.
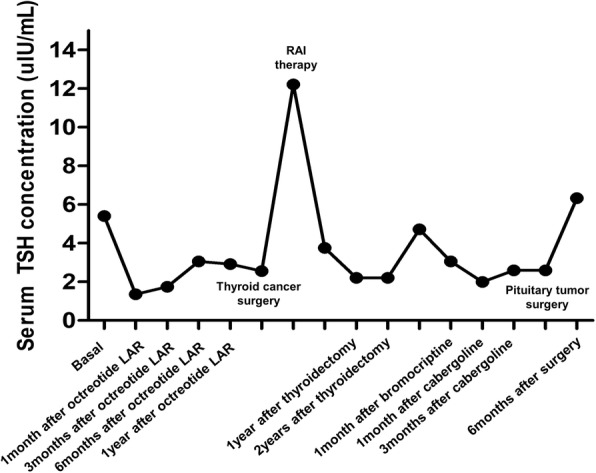
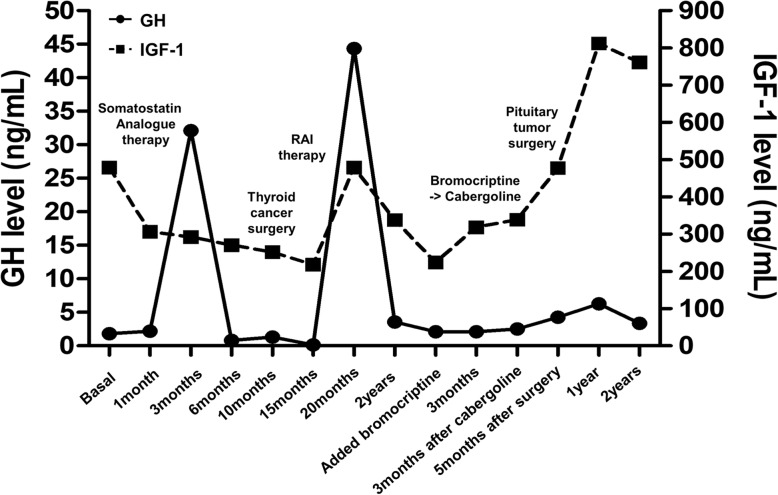
A 59-year-old man was referred to our hospital due to memory impairment and inappropriate TSH level. Sella magnetic resonance imaging revealed a huge pituitary mass extending to the suprasellar area. Clinical diagnosis of TSH/GH co-secreting pituitary adenoma was made based on elevated free T4, total T3, serum α-subunit, insulin-like growth factor-1 levels and non-suppressible GH levels after oral glucose loading. Rectal cancer and multifocal papillary thyroid microcarcinoma (PTMC) were diagnosed during initial screening for internal malignancy; lower anterior resection was performed and close observation was planned for PTMC. Long-acting octreotide therapy was commenced, which resulted in a dramatic reduction in TSHoma size and facilitated control of hormonal excess. Total thyroidectomy and radioactive iodine (RAI) therapy were needed during follow up due to the growth of PTMC. After the surgery, the pituitary adenoma represented resistance to somatostatin analogue therapy and the tumor size gradually increased despite the addition of dopamine agonist therapy. Furthermore, TSH suppressive therapy with levothyroxine was impossible and an adequate TSH level for RAI therapy was unmountable. Late debulking pituitary surgery was ineffective, and the patient gradually deteriorated and lost to follow up.
We report the first aggravated case of TSH/GH co-secreting pituitary tumor after total thyroidectomy for concomitant multifocal PTMC. Deferring of thyroid surgery until the TSHoma is well controlled may be the optimal therapeutic strategy in patients with TSHoma and coexistent thyroid cancer; ablative thyroid surgery may result in catastrophic pituitary tumor growth.
促甲状腺激素(TSH)分泌性垂体腺瘤(TSH 瘤)合并甲状腺癌极为罕见,妥善治疗这两种疾病可能会带来独特的临床挑战。当 TSH 瘤具有多激素性时,特别是同时分泌生长激素(GH)时,治疗可能会更加复杂。本文报告了一例难以治疗的甲状腺癌合并不可治愈的 TSH/GH 分泌性垂体腺瘤病例。
一名 59 岁男性因记忆力减退和 TSH 水平异常而被转至我院。鞍区磁共振成像显示巨大垂体瘤延伸至鞍上区。根据游离 T4、总 T3、血清α亚单位、胰岛素样生长因子-1 水平和口服葡萄糖负荷后不可抑制的 GH 水平升高,临床诊断为 TSH/GH 分泌性垂体腺瘤。在最初筛查内脏恶性肿瘤时,诊断为直肠癌和多灶性甲状腺微小乳头状癌(PTMC);行低位前切除术,计划密切观察 PTMC。长效奥曲肽治疗开始后,TSH 瘤体积显著缩小,激素过度分泌得到控制。由于 PTMC 生长,在随访期间需要行甲状腺全切除术和放射性碘(RAI)治疗。手术后,垂体腺瘤对生长抑素类似物治疗产生抵抗,尽管加用多巴胺激动剂治疗,肿瘤仍逐渐增大。此外,左甲状腺素抑制 TSH 治疗不可能,也无法达到 RAI 治疗的适当 TSH 水平。晚期去瘤垂体手术无效,患者逐渐恶化并失访。
我们报告了首例甲状腺全切除术后并发多灶性 PTMC 后 TSH/GH 分泌性垂体肿瘤加重的病例。对于 TSH 瘤和合并甲状腺癌的患者,延迟甲状腺手术直到 TSH 瘤得到良好控制可能是最佳的治疗策略;甲状腺切除术可能导致灾难性的垂体瘤生长。