Departments of Cardiothoracic Surgery, The Third Xiangya Hospital of Central South University, No. 138 Tongzipo Road, Changsha, 410013, China.
Center for Experimental Medicine, The Third Xiangya Hospital of Central South University, No. 138 Tongzipo Road, Changsha, 410013, China.
World J Surg Oncol. 2021 Aug 30;19(1):258. doi: 10.1186/s12957-021-02364-6.
The standard treatment of stage III N2 small cell lung cancer (SCLC) is concurrent chemoradiation, and surgery is not recommended. This study was aimed to evaluate whether surgery has survival benefits in patients with stage III N2 SCLC and investigate the factors influencing survival of surgery.
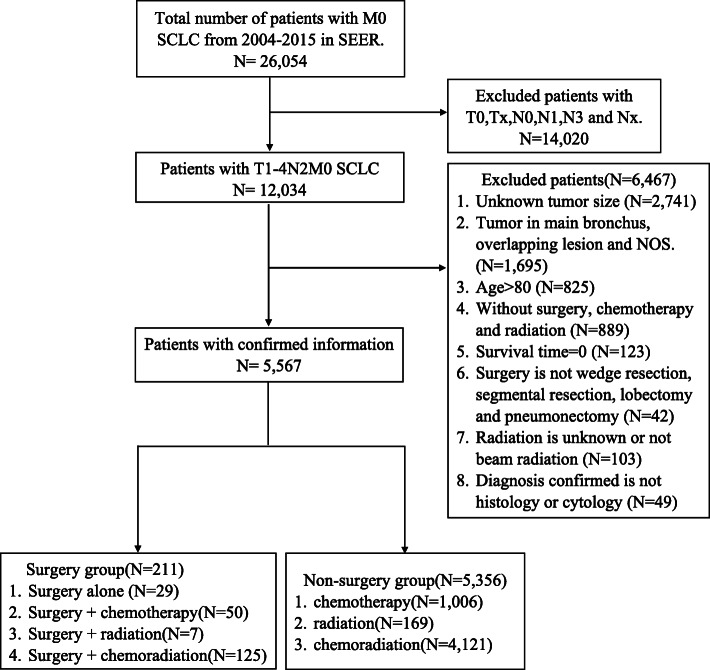
Patients diagnosed with stage T1-4N2M0 SCLC from 2004 to 2015 were selected from the Surveillance Epidemiology End Results database. Propensity score matching (PSM) was used to balance confounders between patients who underwent surgery and those treated with radiation and/or chemotherapy. We compared overall survival (OS) of the two groups using Kaplan-Meier curves and a Cox proportional hazard model. We also identified prognostic factors in patients with surgical resection, and a nomogram was developed and validated for predicting postoperative OS.
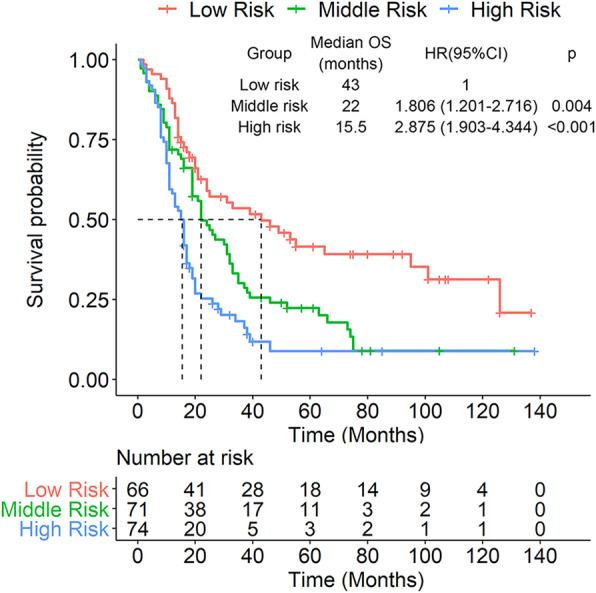
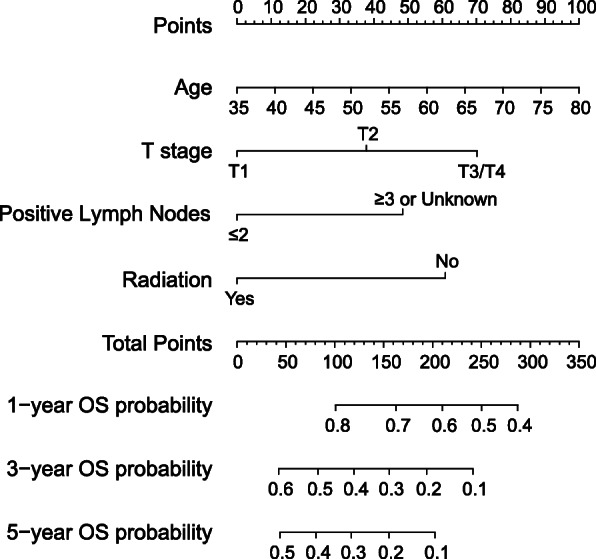
-A total of 5576 patients were included in the analysis; of these, 211 patients underwent surgery. PSM balanced the differences between the two groups. The median OS was longer in the surgery group than in the non-surgery group (20 vs. 15 months; p = 0.0024). Surgery was an independent prognostic factor for longer OS in the multivariate Cox regression analysis, and subgroup analysis revealed a higher survival rate in T1 stage patients treated with surgery (hazard ratio = 0.565, 95% confidence interval: 0.401-0.798; p = 0.001). In patients who underwent surgery, four prognostic factors, including age, T stage, number of positive lymph nodes, and radiation, were selected into nomogram development for predicting postoperative OS. C-index, decision curve analyses, integrated discrimination improvement, and time-dependent receiver operating characteristics showed better performance in nomogram than in the tumor-node-metastasis staging system. Calibration plots demonstrated good consistency between nomogram predicted survival and actual observed survival. The patients were stratified into three different risk groups by prognostic scores and Kaplan-Meier curves showed significant difference between these groups.
These results indicate that surgery can prolong survival in patients with operable stage III N2 SCLC, particularly those with T1 disease. A nomogram that includes age, T stage, number of positive lymph nodes, and radiation can be used to predict their long-term postoperative survival.
局限期 III 期 N2 小细胞肺癌(SCLC)的标准治疗方法是同期放化疗,不推荐手术。本研究旨在评估手术是否能为 III 期 N2 SCLC 患者带来生存获益,并探讨影响手术患者生存的因素。
从 Surveillance, Epidemiology, and End Results(SEER)数据库中选择 2004 年至 2015 年诊断为 T1-4N2M0 SCLC 的患者。采用倾向评分匹配(PSM)平衡手术组和接受放疗和/或化疗组患者之间的混杂因素。我们通过 Kaplan-Meier 曲线和 Cox 比例风险模型比较两组患者的总生存期(OS)。我们还确定了手术切除患者的预后因素,并建立和验证了预测术后 OS 的列线图。
共纳入 5576 例患者,其中 211 例接受手术。PSM 平衡了两组之间的差异。手术组的中位 OS 长于非手术组(20 个月 vs. 15 个月;p=0.0024)。多因素 Cox 回归分析显示,手术是 OS 延长的独立预后因素,亚组分析显示 T1 期患者手术治疗的生存率更高(风险比=0.565,95%置信区间:0.401-0.798;p=0.001)。在接受手术的患者中,年龄、T 分期、阳性淋巴结数和放疗等四个预后因素被选入列线图的开发,以预测术后 OS。C 指数、决策曲线分析、综合判别改善和时间依赖性接受者操作特征曲线显示,列线图在预测术后 OS 方面的表现优于肿瘤-淋巴结-转移分期系统。校准图显示,列线图预测的生存与实际观察到的生存之间具有良好的一致性。根据预后评分将患者分为三个不同的风险组,Kaplan-Meier 曲线显示这些组之间存在显著差异。
这些结果表明,手术可以延长可手术的 III 期 N2 SCLC 患者的生存,特别是 T1 期疾病患者。包含年龄、T 分期、阳性淋巴结数和放疗的列线图可用于预测其长期术后生存。