Sada Ken-Ei, Miyauchi Atsushi, Hashimoto Daisuke, Ino Riku, Nojima Shigeru, Yamanaka Shingo, Kawamura Masafumi
Department of Internal Medicine, Kochi Prefectural Hata-Kenmin Hospital, 3-1Yoshina, Yamanachou, Sukumo, 788-0785, Japan.
Department of Clinical Epidemiology, Kochi Medical School, Kochi University, Nankoku, Japan.
BMC Rheumatol. 2021 Sep 1;5(1):28. doi: 10.1186/s41927-021-00200-8.
Eosinophilic granulomatosis with polyangiitis (EGPA) is an anti-neutrophil antibody (ANCA)-associated necrotizing vasculitis, which predominantly affects small to medium vessels, and is associated with asthma and eosinophilia. EGPA has two different pathogenic aspects: eosinophilic granulomatous inflammation and ANCA-associated inflammation. A recent histological study of peripheral nerves showed that not only ANCA-associated inflammation but also eosinophil-associated vascular occlusion leads to ischemia. Endobronchial involvement is relatively common especially in the patients with granulomatosis with polyangiitis but rare in patients with EGPA. Central nervous system (CNS) involvement is also rare in patients with EGPA, the pathogenesis and relationship between these two rare conditions have not been elucidated.
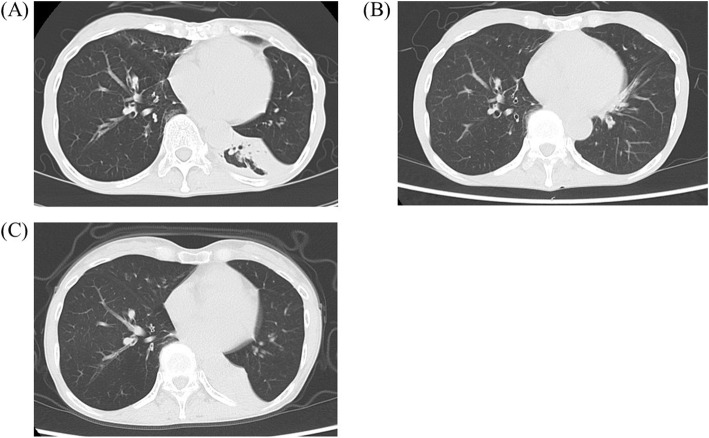
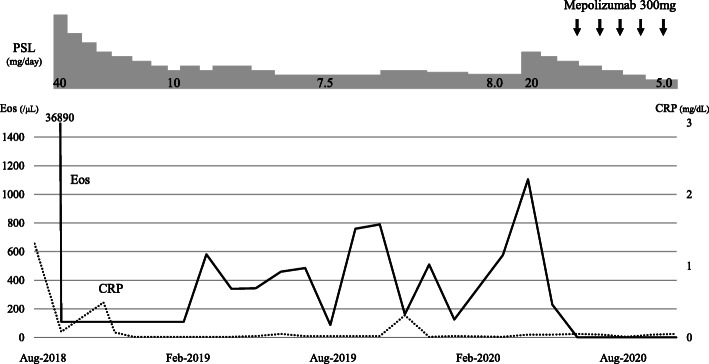
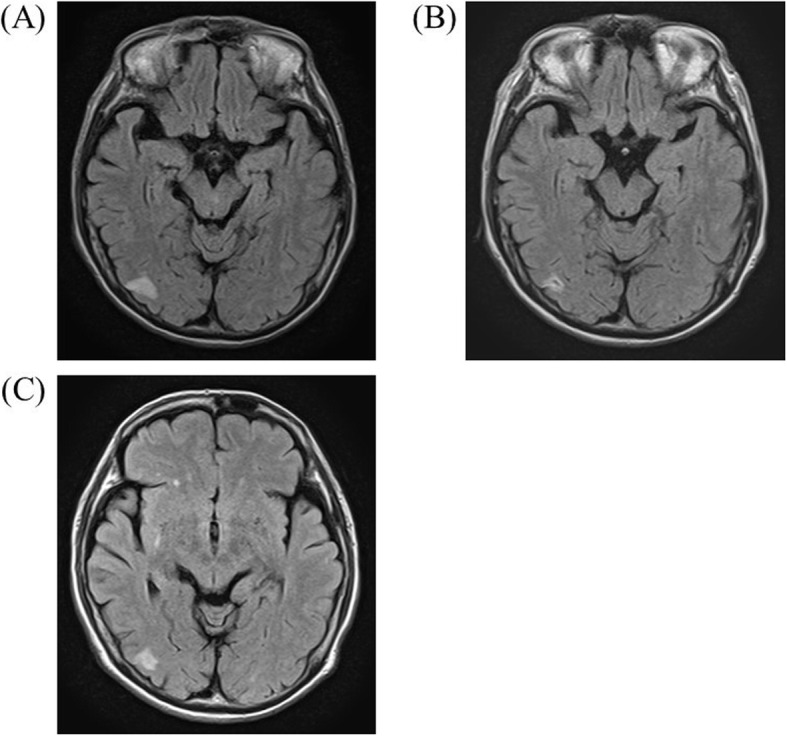
A 62-year-old woman was admitted with numbness, purpura, and eosinophilia. She had a 3-year-history of bronchial asthma. Chest computed tomography showed left lower lobe collapse, and brain magnetic resonance imaging indicated occipital lobe infarction. Skin biopsy findings led to the diagnosis of EGPA. ANCA test results were negative. All symptoms improved after initiating glucocorticoids. However, atelectasis and brain infarction relapsed with increasing eosinophil counts. Atelectasis quickly disappeared with increasing glucocorticoid dose, and glucocorticoid could be reduced to a maintenance dose after the initiation of mepolizumab.
Both atelectasis and brain infarction might develop not only via ANCA-associated inflammation but also via eosinophilic inflammation.
嗜酸性肉芽肿性多血管炎(EGPA)是一种抗中性粒细胞抗体(ANCA)相关的坏死性血管炎,主要累及中小血管,并与哮喘和嗜酸性粒细胞增多有关。EGPA有两个不同的致病方面:嗜酸性肉芽肿性炎症和ANCA相关炎症。最近一项关于周围神经的组织学研究表明,不仅ANCA相关炎症,而且嗜酸性粒细胞相关的血管闭塞都会导致缺血。支气管内受累相对常见,尤其是在肉芽肿性多血管炎患者中,但在EGPA患者中罕见。EGPA患者中枢神经系统(CNS)受累也很罕见,这两种罕见情况的发病机制及其关系尚未阐明。
一名62岁女性因麻木、紫癜和嗜酸性粒细胞增多入院。她有3年支气管哮喘病史。胸部计算机断层扫描显示左肺下叶肺不张,脑部磁共振成像显示枕叶梗死。皮肤活检结果确诊为EGPA。ANCA检测结果为阴性。开始使用糖皮质激素后,所有症状均有改善。然而,随着嗜酸性粒细胞计数增加,肺不张和脑梗死复发。随着糖皮质激素剂量增加,肺不张迅速消失,开始使用美泊利单抗后糖皮质激素可减至维持剂量。
肺不张和脑梗死可能不仅通过ANCA相关炎症,还通过嗜酸性炎症发生。