Department of Cardiothoracic Surgery, New York University Langone Health, New York, New York.
Department of Cardiothoracic Surgery, New York University Langone Health, New York, New York.
Ann Thorac Surg. 2022 Aug;114(2):401-407. doi: 10.1016/j.athoracsur.2021.07.097. Epub 2021 Sep 3.
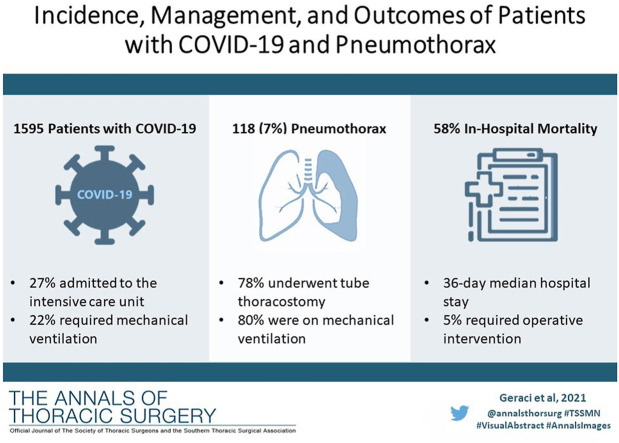
Our objective was to report the incidence, management, and outcomes of patients who developed a secondary pneumothorax while admitted for coronavirus disease 2019 (COVID-19).
A single-institution, retrospective review of patients admitted for COVID-19 with a diagnosis of pneumothorax between March 1, 2020, and April 30, 2020, was performed. The primary assessment was the incidence of pneumothorax. Secondarily, we analyzed clinical outcomes of patients requiring tube thoracostomy, including those requiring operative intervention.
From March 1, 2020, to April 30, 2020, 118 of 1595 patients (7.4%) admitted for COVID-19 developed a pneumothorax. Of these, 92 (5.8%) required tube thoracostomy drainage for a median of 12 days (interquartile range 5-25 days). The majority of patients (95 of 118, 80.5%) were on mechanical ventilation at the time of pneumothorax, 17 (14.4%) were iatrogenic, and 25 patients (21.2%) demonstrated tension physiology. Placement of a large-bore chest tube (20 F or greater) was associated with fewer tube-related complications than a small-bore tube (14 F or less) (14 vs 26 events, P = .011). Six patients with pneumothorax (5.1%) required operative management for a persistent alveolar-pleural fistula. In patients with pneumothorax, median hospital stay was 36 days (interquartile range 20-63 days) and in-hospital mortality was significantly higher than for those without pneumothorax (58% vs 13%, P < .001).
The incidence of secondary pneumothorax in patients admitted for COVID-19 is 7.4%, most commonly occurring in patients requiring mechanical ventilation, and is associated with an in-hospital mortality rate of 58%. Placement of large-bore chest tubes is associated with fewer complications than small-bore tubes.
我们的目的是报告在因 2019 年冠状病毒病(COVID-19)住院期间发生继发性气胸的患者的发病率、处理方法和结局。
对 2020 年 3 月 1 日至 2020 年 4 月 30 日期间因 COVID-19 住院且诊断为气胸的患者进行单中心回顾性研究。主要评估气胸的发病率。其次,我们分析了需要胸腔引流管的患者的临床结局,包括需要手术干预的患者。
2020 年 3 月 1 日至 2020 年 4 月 30 日期间,1595 例 COVID-19 住院患者中有 118 例(7.4%)发生气胸。其中 92 例(5.8%)需要胸腔引流管引流,中位时间为 12 天(四分位距 5-25 天)。大多数患者(118 例中的 95 例,80.5%)在气胸发生时接受机械通气,17 例(14.4%)为医源性气胸,25 例(21.2%)表现为张力性气胸。与小口径(14F 或更小)引流管相比,大口径(20F 或更大)引流管的管相关并发症更少(14 例与 26 例,P=0.011)。6 例气胸患者(5.1%)因持续性肺泡-胸膜瘘需要手术治疗。气胸患者的中位住院时间为 36 天(四分位距 20-63 天),院内死亡率明显高于无气胸患者(58%比 13%,P<0.001)。
COVID-19 住院患者继发性气胸的发生率为 7.4%,最常见于需要机械通气的患者,院内死亡率为 58%。与小口径引流管相比,大口径引流管与更少的并发症相关。