Division of General and Hepatobiliary Surgery, Department of Surgical Sciences, Dentistry, Gynecology and Pediatrics, University of Verona, Verona, Italy.
Section of Radiology, Department of Diagnostic and Public Health, University of Verona, Verona, Italy.
Int J Clin Pract. 2021 Nov;75(11):e14795. doi: 10.1111/ijcp.14795. Epub 2021 Sep 15.
C-reactive protein (CRP) is used for monitoring postoperative inflammation (POI) and detecting infectious complications. The aim of this study was to assess the effect of visceral obesity (VO) on acute POI measured through CRP after elective laparoscopic colorectal resection.
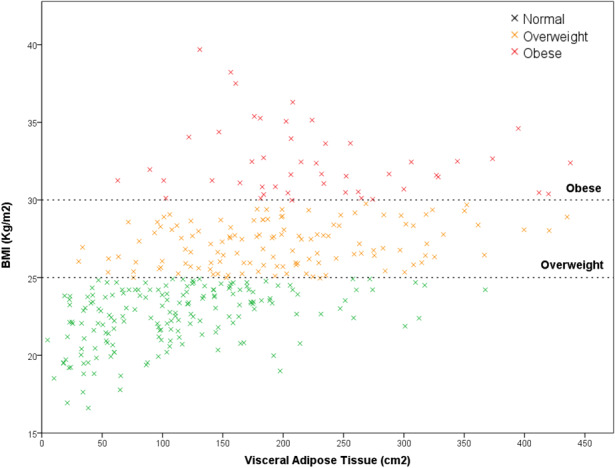
Pre-operative Computed tomography images of 357 patients who underwent laparoscopic colorectal resection were analyzed. Visceral adipose tissue (VAT) area was measured for each patient. VO was defined as VAT area >163.8 cm in men and >80.1 cm in women according to accepted sex-specific cut-offs. Postoperative outcomes and CRP values were compared between VO and non-VO groups. The most appropriate CRP value for identifying infectious complications in the two groups was assessed with receiver operating characteristic (ROC) curves. Univariate and multivariate analyses were conducted for factors affecting POI including VO.
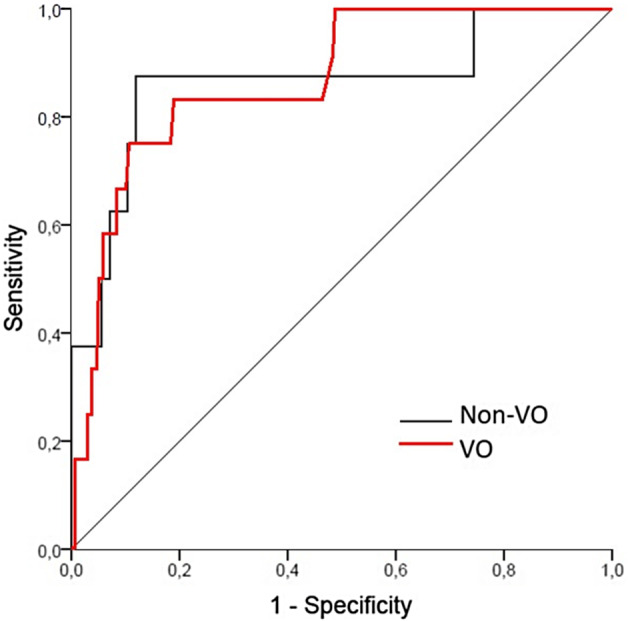
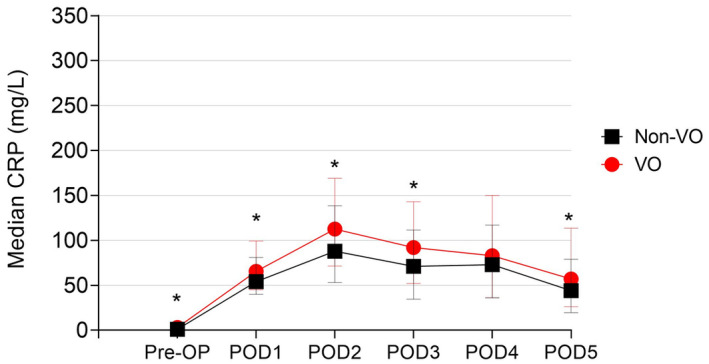
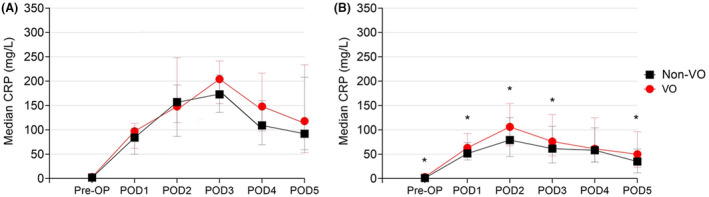
No differences in postoperative outcomes and infectious complications were found in VO patients (62.2% of the overall population). Both in the overall cohort and in patients without infectious complications, VO was associated with higher CRP values on postoperative day (POD) 1, POD2, POD3, and POD5. A positive correlation was found between VAT and CRP on all PODs. VO independently predicted higher CRP on POD1-3 in patients without infectious complications but not in those who developed complications. ROC curves analysis showed optimal accuracy for detection of infectious complications for CRP on POD3 in both groups, though the optimal cut-off value was higher in VO group (154 vs 136 mg/L).
VO is not associated to increased complications after laparoscopic colorectal resection. Nevertheless, it is independently associated to higher CRP in the overall population and in patients without infectious complications. Consequently, CRP values on POD3 higher than cut-offs commonly adopted in the clinical practice should be carefully evaluated in VO patients to assess the occurrence of infectious complications.
C 反应蛋白(CRP)用于监测术后炎症(POI)并检测感染性并发症。本研究旨在评估内脏肥胖(VO)对择期腹腔镜结直肠切除术后通过 CRP 测量的急性 POI 的影响。
分析了 357 例接受腹腔镜结直肠切除术患者的术前计算机断层扫描图像。为每位患者测量内脏脂肪组织(VAT)面积。根据公认的性别特异性截止值,将 VAT 面积男性>163.8cm 和女性>80.1cm 定义为 VO。比较 VO 和非 VO 组之间的术后结果和 CRP 值。使用接收者操作特征(ROC)曲线评估两组中用于识别感染性并发症的最佳 CRP 值。对影响包括 VO 在内的 POI 的因素进行单变量和多变量分析。
在 VO 患者中(总体人群的 62.2%),术后结果和感染性并发症无差异。在整个队列和无感染性并发症的患者中,VO 与术后第 1、2、3 和 5 天的 CRP 值较高相关。在所有 POD 上均发现 VAT 与 CRP 呈正相关。在无感染性并发症的患者中,VO 独立预测了 POD1-3 时 CRP 值较高,但在发生并发症的患者中则没有。ROC 曲线分析显示,两组中 CRP 在 POD3 时检测感染性并发症的准确性最佳,尽管 VO 组的最佳截断值较高(154 比 136mg/L)。
VO 与腹腔镜结直肠切除术后并发症增加无关。然而,它与整个人群和无感染性并发症患者的 CRP 升高独立相关。因此,在 VO 患者中,CRP 值高于临床实践中常用的截断值时,应仔细评估是否发生感染性并发症。