Department of Medicine, Surgery and Dentistry, University of Salerno, Baronissi, Salerno, Italy.
Department of Chemistry and Biology, University of Salerno, Fisciano, Italy.
Oxid Med Cell Longev. 2021 Aug 30;2021:4936571. doi: 10.1155/2021/4936571. eCollection 2021.
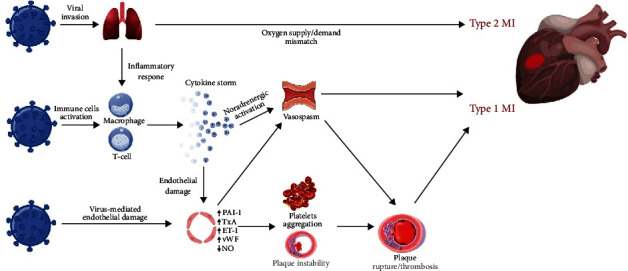
Acute coronary syndromes (ACS) are frequently reported in patients with coronavirus disease 2019 (COVID-19) and may impact patient clinical course and mortality. Although the underlying pathogenesis remains unclear, several potential mechanisms have been hypothesized, including oxygen supply/demand imbalance, direct viral cellular damage, systemic inflammatory response with cytokine-mediated injury, microvascular thrombosis, and endothelial dysfunction. The severe hypoxic state, combined with other conditions frequently reported in COVID-19, namely sepsis, tachyarrhythmias, anemia, hypotension, and shock, can induce a myocardial damage due to the mismatch between oxygen supply and demand and results in type 2 myocardial infarction (MI). In addition, COVID-19 promotes atherosclerotic plaque instability and thrombus formation and may precipitate type 1 MI. Patients with severe disease often show decrease in platelets count, higher levels of d-dimer, ultralarge von Willebrand factor multimers, tissue factor, and prolongation of prothrombin time, which reflects a prothrombotic state. An endothelial dysfunction has been described as a consequence of the direct viral effects and of the hyperinflammatory environment. The expression of tissue factor, von Willebrand factor, thromboxane, and plasminogen activator inhibitor-1 promotes the prothrombotic status. In addition, endothelial cells generate superoxide anions, with enhanced local oxidative stress, and endothelin-1, which affects the vasodilator/vasoconstrictor balance and platelet aggregation. The optimal management of COVID-19 patients is a challenge both for logistic and clinical reasons. A deeper understanding of ACS pathophysiology may yield novel research insights and therapeutic perspectives in higher cardiovascular risk subjects with COVID-19.
急性冠状动脉综合征(ACS)在新型冠状病毒病 2019(COVID-19)患者中经常报告,可能影响患者的临床病程和死亡率。尽管其潜在发病机制尚不清楚,但已经假设了几种潜在机制,包括氧供需失衡、病毒直接细胞损伤、细胞因子介导损伤的全身炎症反应、微血管血栓形成和内皮功能障碍。严重的低氧状态,加上 COVID-19 中经常报告的其他情况,即败血症、心动过速、贫血、低血压和休克,可由于氧供与氧需之间的不匹配而导致心肌损伤,并导致 2 型心肌梗死(MI)。此外,COVID-19 可促进动脉粥样硬化斑块不稳定和血栓形成,并可能引发 1 型 MI。重症患者常表现为血小板计数下降、D-二聚体水平升高、超大 von Willebrand 因子多聚体、组织因子和凝血酶原时间延长,反映出一种血栓形成状态。内皮功能障碍被描述为直接病毒作用和过度炎症环境的结果。组织因子、von Willebrand 因子、血栓素和纤溶酶原激活物抑制剂-1 的表达促进了血栓形成状态。此外,内皮细胞产生超氧阴离子,局部氧化应激增强,内皮素-1 影响血管舒张/收缩平衡和血小板聚集。COVID-19 患者的最佳管理既是出于后勤原因,也是出于临床原因的挑战。深入了解 ACS 病理生理学可能会为 COVID-19 中心血管风险较高的患者提供新的研究见解和治疗观点。