Academic Unit of Bone Metabolism, University of Sheffield, Sheffield, UK.
Department of Epidemiology & Biostatistics, University of California, San Francisco, San Francisco, CA, USA.
J Bone Miner Res. 2022 Jan;37(1):29-35. doi: 10.1002/jbmr.4433. Epub 2021 Sep 24.
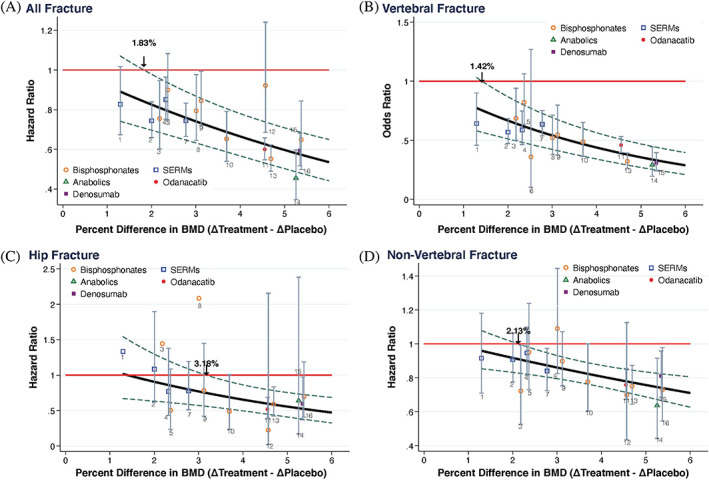
The surrogate threshold effect (STE) is defined as the minimum treatment effect on a surrogate that is reliably predictive of a treatment effect on the clinical outcome. It provides a framework for implementing a clinical trial with a surrogate endpoint. The aim of this study was to update our previous analysis by validating the STE for change in total hip (TH) BMD as a surrogate for fracture risk reduction; the novelty of this study was this validation. To do so, we used individual patient data from 61,415 participants in 16 RCTs that evaluated bisphosphonates (nine trials), selective estrogen receptor modulators (four trials), denosumab (one trial), odanacatib (one trial), and teriparatide (one trial) to estimate trial-specific treatment effects on TH BMD and all, vertebral, hip, and nonvertebral fractures. We then conducted a random effects meta-regression of the log relative fracture risk reduction against 24-month change in TH BMD, and computed the STE as the intersection of the upper 95% prediction limit of this regression with the line of no fracture reduction. We validated the STE by checking whether the number of fractures in each trial provided 80% power and determining what proportion of trials with BMD changes ≥ STE reported significant reductions in fracture risk. We applied this analysis to (i) the trials on which we estimated the STE; and (ii) trials on which we did not estimate the STE. We found that the STEs for all, vertebral, hip, and nonvertebral fractures were 1.83%, 1.42%, 3.18%, and 2.13%, respectively. Among trials used to estimate STE, 27 of 28 were adequately powered, showed BMD effects exceeding the STE, and showed significant reductions in fracture risk. Among the validation set of 11 trials, 10 met these criteria. Thus STE differs by fracture type and has been validated in trials not used to develop the approach. © 2021 The Authors. Journal of Bone and Mineral Research published by Wiley Periodicals LLC on behalf of American Society for Bone and Mineral Research (ASBMR).
替代终点阈值效应(STE)定义为替代终点有可靠预测治疗效果的最小治疗效果。它为使用替代终点进行临床试验提供了一个框架。本研究的目的是通过验证全髋关节(TH)骨密度变化作为骨折风险降低的替代终点的 STE 来更新我们之前的分析;本研究的新颖之处在于验证了这一点。为此,我们使用了来自 16 项随机对照试验的 61415 名参与者的个体患者数据,这些试验评估了双膦酸盐(9 项试验)、选择性雌激素受体调节剂(4 项试验)、地诺单抗(1 项试验)、odanacatib(1 项试验)和特立帕肽(1 项试验),以估计每种治疗方法对 TH 骨密度和所有、椎体、髋部和非椎体骨折的治疗效果。然后,我们对 24 个月时 TH 骨密度变化与相对骨折风险降低的对数进行了随机效应荟萃回归,并将 STE 计算为该回归的上 95%预测限与无骨折降低线的交点。我们通过检查每个试验中的骨折数量是否提供 80%的功效,并确定有多少骨密度变化≥STE 的试验报告骨折风险显著降低,来验证 STE。我们将此分析应用于(i)我们估计 STE 的试验;和(ii)我们没有估计 STE 的试验。我们发现,所有、椎体、髋部和非椎体骨折的 STE 分别为 1.83%、1.42%、3.18%和 2.13%。在用于估计 STE 的试验中,28 项中的 27 项具有足够的功效,显示出骨密度效应超过 STE,并且骨折风险显著降低。在 11 项验证试验中,有 10 项符合这些标准。因此,STE 因骨折类型而异,并已在未用于开发该方法的试验中得到验证。© 2021 作者。骨与矿物研究杂志由 Wiley 期刊公司代表美国骨与矿物研究协会(ASBMR)出版。