Department of Orthopaedic Surgery, Beijing Jishuitan Hospital, Fourth Clinical College of Peking University, Beijing, China.
Tian Ji Laboratory, Beijing Tinavi Medical Technology Co., Beijing, China.
Clin Orthop Relat Res. 2022 Jan 1;480(1):191-205. doi: 10.1097/CORR.0000000000001923.
Lumbar-pelvic stiffness and sagittal imbalance have been reported to increase the risk of dislocation and wear after THA. One potential way to approach this concern is by identifying patient-specific safe zones for THA components based on the standing and sitting sagittal pelvic tilt. However, there is no algorithm to integrate the standing and sitting pelvic tilt into the surgical plan of component orientations.
QUESTIONS/PURPOSES: We established a new mathematical algorithm for determining a patient-specific safe zone for THA by integrating the impingement-free ROM requirements of standing and sitting while preventing edge loading while standing. We aimed to determine (1) the accuracy of this new method for predicting the impingement-free ROM for a given component orientation, (2) the sensitivity and specificity of detecting an impingement-free acetabular cup position for standing and sitting, and (3) the influences of key factors including pelvic tilt while standing and pelvic tilt while sitting and implant parameters on patient-specific safe zones.
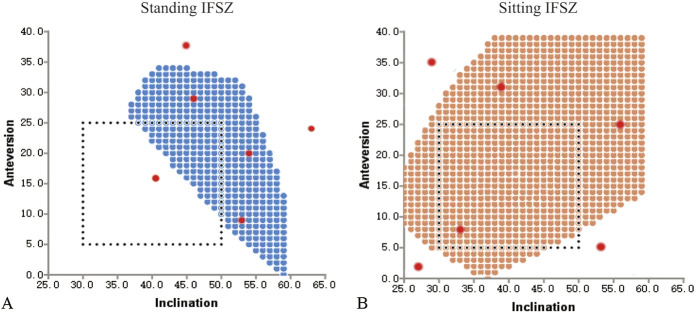
A strategy for calculating the intersection of standing and sitting impingement-free safe zones and the zone of a standing radiographic inclination of ≤ 45° was used to develop patient-specific safe zones. We conducted a computer simulation study including the pelvis and THA prosthesis to answer the three study questions. We enrolled 10 patients who underwent robot-assisted THA for avascular necrosis of the femoral head (mean age 49 ± 19 years; five were women) from October 2019 to December 2019. We used a prosthesis model with a conical stem neck and a non-hooded liner, with the femoral head diameter ranging between 28 mm and 40 mm, and the corresponding head-neck ratio ranging between 2.33 and 3.33. We tested 1680 movements for the accuracy of impingement-free ROM (Question 1), and 80 marginal points and 120 non-marginal points of the comprehensive impingement-free safe zone, which combines the standing and sitting postures (Question 2). For Question 3, we explored the influences of standing and sitting pelvic tilt, femoral head diameter, and ROM criteria on the size of the patient-specific safe zone.
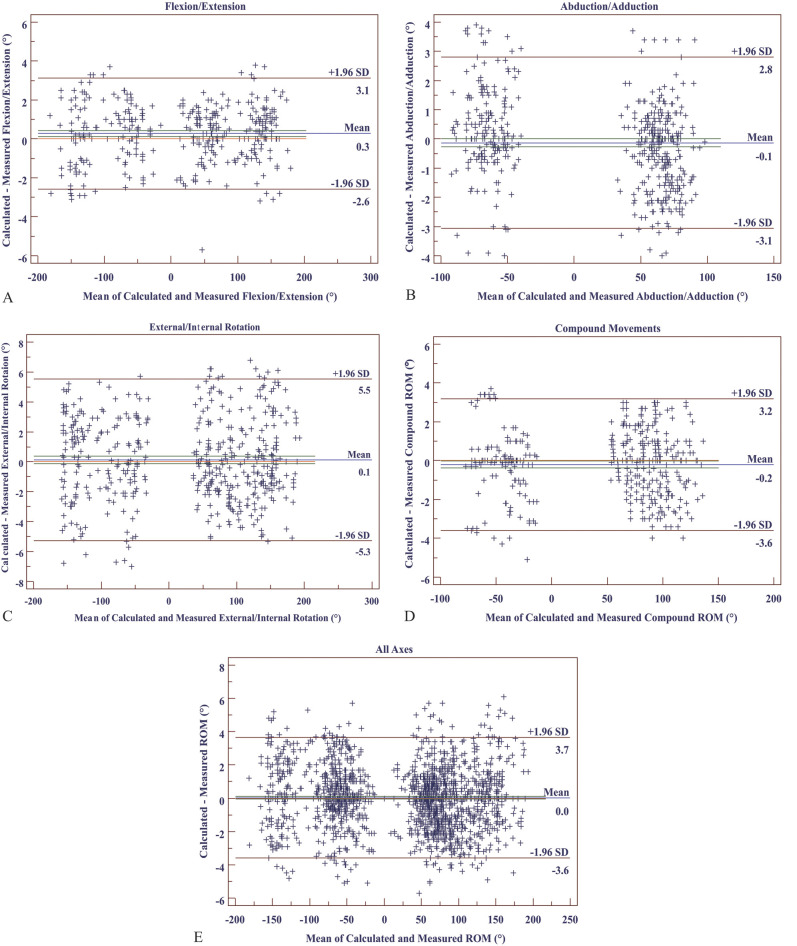
With the simulation method as a reference for detecting impingement, the mean absolute error (arithmetic mean of all the absolute errors) of the calculated impingement-free ROM was 1.4° ± 2.3°, and the limit of agreement of errors was between -3.6° and 3.7°. The sensitivity of detecting a safe cup orientation within the comprehensive impingement-free safe zone for a given ROM criterion was 98.9% (95% CI 93.6% to 99.9%), and specificity was 97.1% (95% CI 91.0% to 99.2%). There were no impingement-free safe zones for 29% (pelvic tilt combinations without an impingement-free safe zone and all tested combinations) and no patient-specific safe zones for 46% (pelvic tilt combinations without a patient-specific safe zone and all tested combinations) of the tested combinations of standing and sitting pelvic tilt. The patient-specific safe zone was sensitive to changes in standing and sitting pelvic tilt, femoral head diameter, stem version, and ROM criteria. Stem anteversions beyond 10° to 20° dramatically reduced the size of the patient-specific safe zone to 0 within a change of 10° to 20°.
The patient-specific safe zone algorithm can be an accurate method for determining the optimal orientation for acetabular cups and femoral stems in THA. The patient-specific safe zone is sensitive to changes in standing and sitting pelvic tilt, stem version, ROM criteria, and the femoral head diameter. A narrow zone of 10° to 20° for stem anteversion is recommended to maximize the size of the patient-specific safe zone.
This study suggests the potential of a mathematical algorithm to optimize the orientation of THA components and illustrates how key parameters affect the patient-specific safe zone.
腰椎骨盆僵硬和矢状面失衡已被报道会增加髋关节置换术后脱位和磨损的风险。一种潜在的方法是通过确定基于站立和坐姿骨盆倾斜的髋关节置换组件的特定患者安全区域来解决这个问题。然而,目前还没有算法可以将站立和坐姿骨盆倾斜整合到手术计划的组件方向中。
问题/目的:我们建立了一种新的数学算法,通过整合站立和坐姿的无撞击活动范围要求,同时防止站立时的边缘负荷,来确定髋关节置换术的特定患者安全区域。我们旨在确定(1)该新方法预测特定患者安全区域的准确性,(2)检测站立和坐姿无撞击髋臼杯位置的敏感性和特异性,(3)站立和坐姿骨盆倾斜以及植入物参数等关键因素对特定患者安全区域的影响。
使用计算站立和坐姿无撞击安全区域的交集以及站立时放射学倾斜角度≤45°的区域的策略来开发特定患者的安全区域。我们进行了一项计算机模拟研究,包括骨盆和髋关节置换假体,以回答三个研究问题。我们招募了 10 名因股骨头缺血性坏死而接受机器人辅助髋关节置换术的患者(平均年龄 49±19 岁;五名为女性),研究时间为 2019 年 10 月至 2019 年 12 月。我们使用了一种带有锥形柄颈和无罩衬垫的假体模型,股骨头直径在 28mm 到 40mm 之间,头颈比在 2.33 到 3.33 之间。我们测试了 1680 个运动来确定无撞击活动范围的准确性(问题 1),并测试了综合无撞击安全区域的 80 个边缘点和 120 个非边缘点(问题 2)。对于问题 3,我们探讨了站立和坐姿骨盆倾斜、股骨头直径和活动范围标准对特定患者安全区域大小的影响。
以模拟方法作为检测撞击的参考,计算出的无撞击活动范围的平均绝对误差(所有绝对误差的算术平均值)为 1.4°±2.3°,误差的一致性限在-3.6°和 3.7°之间。在给定活动范围标准的情况下,检测综合无撞击安全区域内安全杯位置的敏感性为 98.9%(95%置信区间为 93.6%至 99.9%),特异性为 97.1%(95%置信区间为 91.0%至 99.2%)。在测试的站立和坐姿骨盆倾斜组合中,有 29%(没有无撞击安全区域的骨盆倾斜组合和所有测试组合)和 46%(没有特定患者安全区域的骨盆倾斜组合和所有测试组合)没有无撞击安全区域。特定患者安全区域对站立和坐姿骨盆倾斜、股骨头直径、柄版本和活动范围标准的变化敏感。在 10°至 20°的范围内,柄前倾角的变化超过 10°至 20°,会使特定患者安全区域的大小急剧缩小到 0。
特定患者安全区域算法可以成为确定髋关节置换髋臼杯和股骨柄最佳方向的准确方法。特定患者安全区域对站立和坐姿骨盆倾斜、柄版本、活动范围标准和股骨头直径的变化敏感。建议使用 10°至 20°的柄前倾角窄范围,以最大限度地扩大特定患者安全区域的大小。
本研究表明,一种数学算法有可能优化髋关节置换组件的方向,并说明了关键参数如何影响特定患者的安全区域。