Miuli Andrea, Sepede Gianna, Stigliano Gianfranco, Mosca Alessio, Di Carlo Francesco, d'Andrea Giacomo, Lalli Aliseo, Spano Maria Chiara, Pettorruso Mauro, Martinotti Giovanni, di Giannantonio Massimo
Department of Neuroscience, Imaging and Clinical Sciences, "G. d'Annunzio" University of Chieti, Chieti 66100, Italy.
Department of Psychiatry Affective Neuropsychiatry, Sahlgrenska University Hospital, Göteborg 40530, Sweden.
World J Psychiatry. 2021 Aug 19;11(8):477-490. doi: 10.5498/wjp.v11.i8.477.
Nowadays there is an increasing use of transcranial magnetic stimulation (TMS) both in neurological and psychiatric fields. After Food and Drug Administration approval of TMS for the therapy of treatment-resistant depression, TMS has been widely used in the context of mood disorders (MD). However, growing reports regarding the possibility of developing hypomanic/manic switch (HMS) have generated concern regarding its use in MDs.
To investigate the actual risk of developing HMS due to TMS in the treatment of MD.
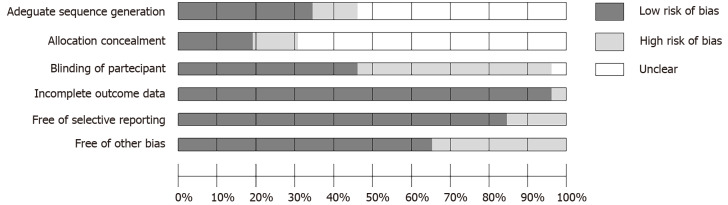
We led our research on PubMed, Scopus and Web of Science on March 22, 2020, in accordance to the PRISMA guidelines for systematic review. Only double blind/single blind studies, written in English and focused on the TMS treatment of MD, were included. A meta-analysis of repetitive TMS protocol studies including HMS was conducted using RevMan 5.4 software. The assessment of Risk of Bias was done using Cochrane risk of bias tool. This protocol was registered on PROSPERO with the CRD42020175811 code.
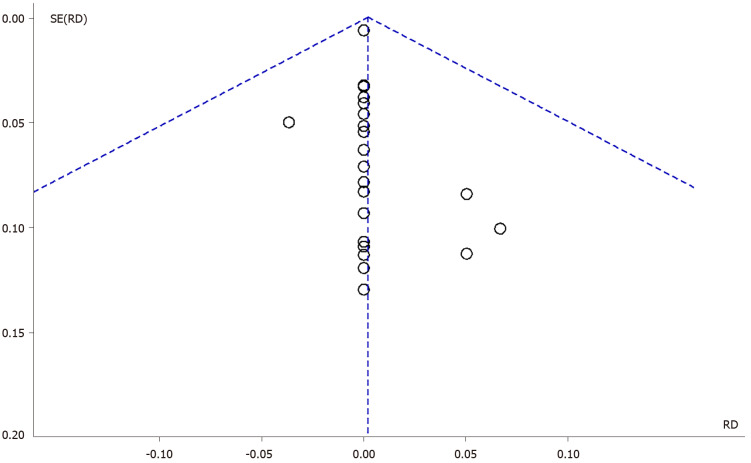
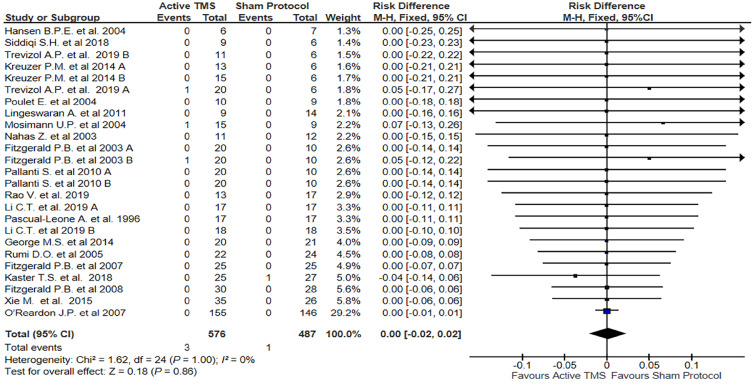
Twenty-five studies were included in our meta-analysis: Twenty-one double blind randomized controlled trials (RCT) and four single blind-RCT (no. of subjects involved in active stimulation = 576; no. of subjects involved in sham protocol = 487). The most frequently treated pathology was major depressive episode/major depressive disorder, followed by resistant depression, bipolar depression and other MD. The majority of the studies used a repetitive TMS protocol, and the left dorsolateral prefrontal cortex was the main target area. Side effects were reported in eight studies and HMS (described as greater energy, insomnia, irritability, anxiety, suicidal attempt) in four studies. When comparing active TMS sham treatment, the risk of developing HMS was not significantly different between conditions.
Applying the most usual protocols and the appropriate precautionary measures, TMS seems not to be related to HMS development.
如今,经颅磁刺激(TMS)在神经科和精神科领域的应用越来越广泛。在美国食品药品监督管理局批准TMS用于治疗难治性抑郁症后,TMS已在情绪障碍(MD)的治疗中广泛应用。然而,越来越多关于发生轻躁狂/躁狂转换(HMS)可能性的报告引发了人们对其在MD治疗中应用的担忧。
探讨MD治疗中TMS导致HMS的实际风险。
我们于2020年3月22日按照系统评价的PRISMA指南在PubMed、Scopus和Web of Science上开展研究。仅纳入以英文撰写、聚焦于MD的TMS治疗的双盲/单盲研究。使用RevMan 5.4软件对包括HMS的重复TMS方案研究进行荟萃分析。使用Cochrane偏倚风险工具进行偏倚风险评估。该方案已在PROSPERO上注册,注册号为CRD42020175811。
25项研究纳入我们的荟萃分析:21项双盲随机对照试验(RCT)和4项单盲RCT(接受主动刺激的受试者数量 = 576;接受假刺激方案的受试者数量 = 487)。最常治疗的疾病是重度抑郁发作/重度抑郁症,其次是难治性抑郁症、双相抑郁症和其他MD。大多数研究使用重复TMS方案,左侧背外侧前额叶皮质是主要靶区。8项研究报告了副作用,4项研究报告了HMS(表现为精力更充沛、失眠、易怒、焦虑、自杀企图)。比较主动TMS与假刺激治疗时,不同治疗条件下发生HMS的风险无显著差异。
应用最常用的方案并采取适当的预防措施,TMS似乎与HMS的发生无关。