Radboud Institute for Health Sciences, Amalia Children's Hospital, Department of Paediatrics, Division of Neonatology, Radboud University Medical Centre Nijmegen, Internal postal code 804, Geert Grooteplein Zuid 10, 6525, GA, Nijmegen, The Netherlands.
Department for Health Evidence, Radboud University Medical Centre, Geert Grooteplein Zuid 10, 6525, GA, Nijmegen, The Netherlands.
Trials. 2021 Sep 15;22(1):627. doi: 10.1186/s13063-021-05594-x.
Controversy exists about the optimal management of a patent ductus arteriosus (PDA) in preterm infants. A persistent PDA is associated with neonatal mortality and morbidity, but causality remains unproven. Although both pharmacological and/or surgical treatment are effective in PDA closure, this has not resulted in an improved neonatal outcome. In most preterm infants, a PDA will eventually close spontaneously, hence PDA treatment potentially increases the risk of iatrogenic adverse effects. Therefore, expectant management is gaining interest, even in the absence of convincing evidence to support this strategy.
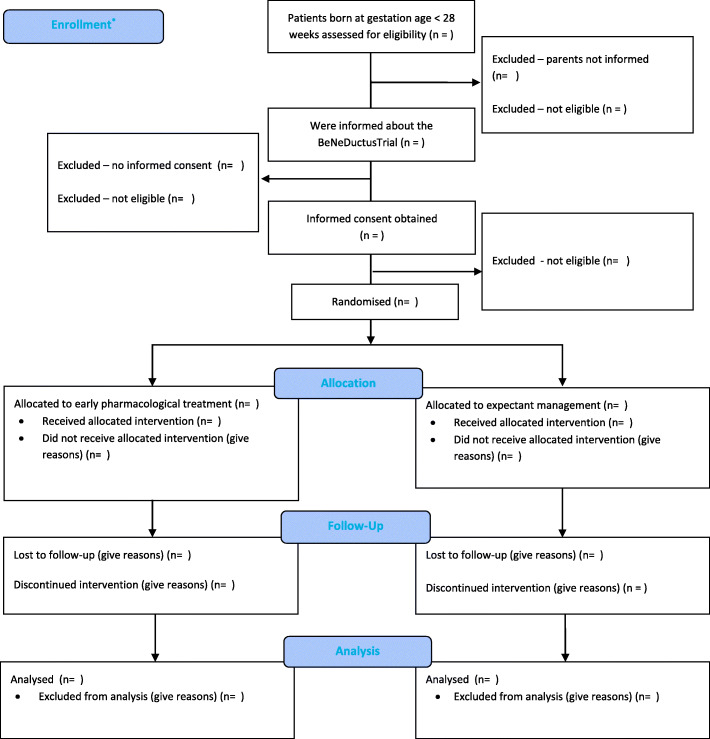
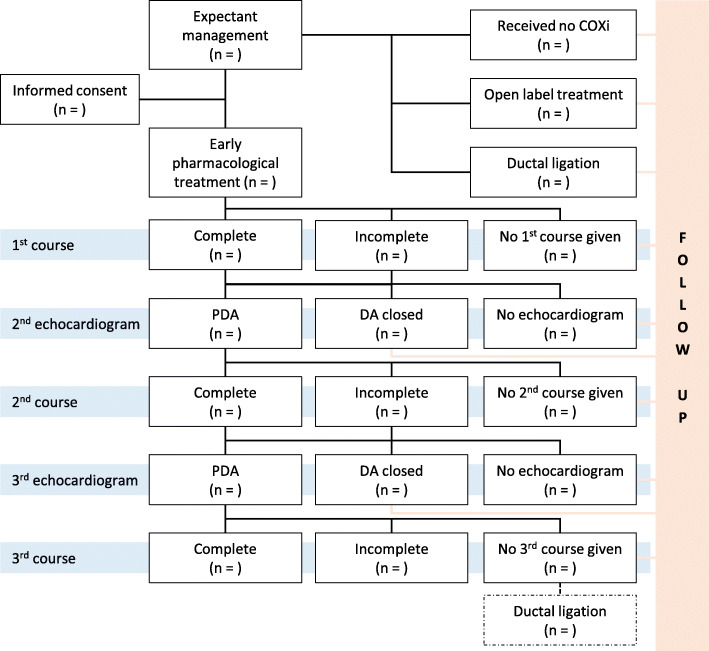
METHODS/DESIGN: The BeNeDuctus trial is a multicentre, randomised, non-inferiority trial assessing early pharmacological treatment (24-72 h postnatal age) with ibuprofen versus expectant management of PDA in preterm infants in Europe. Preterm infants with a gestational age of less than 28 weeks and an echocardiographic-confirmed PDA with a transductal diameter of > 1.5 mm are randomly allocated to early pharmacological treatment with ibuprofen or expectant management after parental informed consent. The primary outcome measure is the composite outcome of mortality, and/or necrotizing enterocolitis Bell stage ≥ IIa, and/or bronchopulmonary dysplasia, all established at a postmenstrual age of 36 weeks. Secondary short-term outcomes are comorbidity and adverse events assessed during hospitalization and long-term neurodevelopmental outcome assessed at a corrected age of 2 years. This statistical analysis plan focusses on the short-term outcome and is written and submitted without knowledge of the data.
ClinicalTrials.gov NTR5479. Registered on October 19, 2015, with the Dutch Trial Registry, sponsored by the United States National Library of Medicine Clinicaltrials.gov NCT02884219 (registered May 2016) and the European Clinical Trials Database EudraCT 2017-001376-28.
早产儿动脉导管未闭(PDA)的最佳治疗方法存在争议。持续性 PDA 与新生儿死亡率和发病率有关,但因果关系尚未得到证实。虽然药物和/或手术治疗均可有效关闭 PDA,但这并未改善新生儿结局。在大多数早产儿中,PDA 最终会自行关闭,因此 PDA 治疗可能会增加医源性不良反应的风险。因此,期待治疗方法越来越受到关注,即使缺乏支持这种策略的令人信服的证据。
方法/设计:BeNeDuctus 试验是一项多中心、随机、非劣效性试验,评估了在欧洲早产儿中,与期待治疗相比,在生后 24-72 小时使用布洛芬进行早期药物治疗对 PDA 的疗效。胎龄<28 周且经超声心动图证实存在 PDA(跨导管直径>1.5 毫米)的早产儿,在获得家长知情同意后,随机分配至早期使用布洛芬进行药物治疗或期待治疗。主要结局指标是死亡,以及/或坏死性小肠结肠炎 Bell 分级≥Ⅱa,和/或支气管肺发育不良的复合结局,所有结局均在校正胎龄 36 周时评估。次要短期结局是住院期间的合并症和不良事件,以及校正年龄 2 岁时的长期神经发育结局。本统计分析计划重点关注短期结局,在不了解数据的情况下编写和提交。
ClinicalTrials.gov NTR5479. 于 2015 年 10 月 19 日在荷兰临床试验注册中心注册,由美国国家医学图书馆临床研究.gov NCT02884219(2016 年 5 月注册)和欧洲临床试验数据库 EudraCT 2017-001376-28 资助。