Soto Maria Elena, Ochoa-Hein Eric, Anaya-Ayala Javier E, Ayala-Picazo Micaela, Koretzky Solange Gabriela
Instituto Nacional de Cardiologia Ignacio Chavez, Mexico City, México.
American British Cowdray Medical Center, Mexico City, México.
J Thorac Dis. 2021 Aug;13(8):4830-4844. doi: 10.21037/jtd-21-789.
Aortic aneurysm and dissection are important causes of morbimortality in patients with Marfan syndrome (MFS) and other connective tissue diseases that affect the cardiovascular tissues. Timely intervention through different surgical techniques improves the prognosis. Both sparing and replacement-type interventions of the aortic valve are used, but selection depends on the condition of the patient at the time of diagnosis, the patient's emergency condition, surgeon preference and hospital resources. Previous meta-analyses have suggested an advantage with the use of sparing-type interventions, but this finding must be updated and extended to patients with other connective tissue disorders. The objetive of this study is to evaluate the outcomes of valve-sparing root replacement versus aortic root replacement procedures in patients with MFS and similar connective tissue diseases that present with aortic aneurysm or dissection.
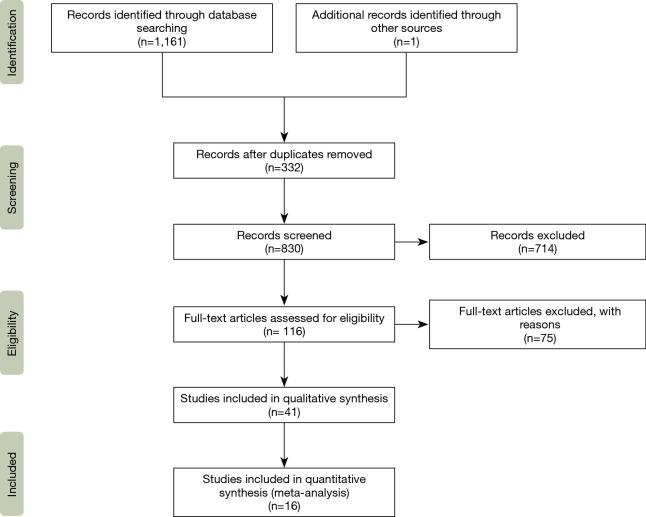
A systematic review of cohort studies that evaluated sparing-type (preserving, remodeling, reimplantation, Yacoub, David or Florida Sleeve) or replacement-type (repair, Bentall, Button-Bentall, composite valve graft or Cabrol) procedures in patients with Marfan, Loeys-Dietz, Beals-Hecht or Ehlers-Danlos syndromes was done. Studies were retrieved from the SCOPUS, MEDLINE, CINAHL, EMBASE and LILACS electronic databases up to January 2020 without language restrictions. Only studies that directly compared sparing- versus replacement-type procedures were included in the meta-analysis.
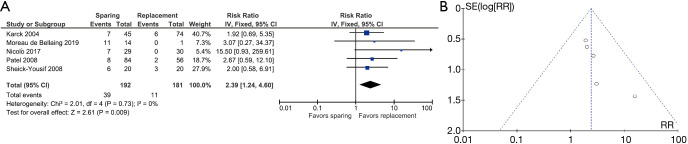
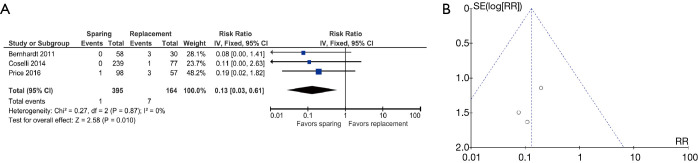
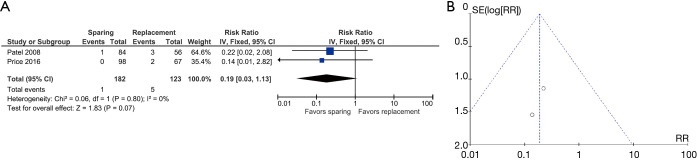
A total of 33 studies (n=1,807 subjects) reported sparing-type surgical interventions and 26 studies (n=2,218 subjects) reported replacement-type surgical interventions. Pooled rates of endocarditis, thromboembolism and aneurysm were higher in replacement-type surgical intervention studies. Sixteen studies were included in the meta-analysis. Sparing-type interventions were associated with a reduced risk of endocarditis (RR =0.13, 95% CI: 0.03-0.61); however, replacement-type interventions favored freedom from valve reoperation (RR =2.39, 95% CI: 1.24-4.60). All studies were at low risk of bias.
The choice of the best surgical technique is dependent on the type of disease (MFS or other connective tissue diseases) as well as the accompanying aortic and cardiovascular damage, since these key factors are heterogeneous. Although the results of this meta-analysis tend to show some advantages for one type of surgical intervention over the other and viceversa, the surgeon can only make the best decision during the surgical act.
主动脉瘤和主动脉夹层是马凡综合征(MFS)及其他影响心血管组织的结缔组织疾病患者发病和死亡的重要原因。通过不同的手术技术进行及时干预可改善预后。主动脉瓣的保留和置换型干预均有应用,但选择取决于诊断时患者的状况、患者的紧急情况、外科医生的偏好和医院资源。以往的荟萃分析表明保留型干预具有优势,但这一发现必须更新并扩展到患有其他结缔组织疾病的患者。本研究的目的是评估在患有MFS及伴有主动脉瘤或主动脉夹层的类似结缔组织疾病的患者中,保留瓣膜根部置换术与主动脉根部置换术的疗效。
对队列研究进行系统评价,这些研究评估了马凡综合征、洛伊茨-迪茨综合征、比尔斯-赫希综合征或埃勒斯-当洛综合征患者的保留型(保留、重塑、再植入、亚库布、大卫或佛罗里达袖套)或置换型(修复、本塔尔、纽扣-本塔尔、复合瓣膜移植或卡布罗尔)手术。从SCOPUS、MEDLINE、CINAHL、EMBASE和LILACS电子数据库中检索截至2020年1月的研究,无语言限制。荟萃分析仅纳入直接比较保留型与置换型手术的研究。
共有33项研究(n = 1807名受试者)报告了保留型手术干预,26项研究(n = 2218名受试者)报告了置换型手术干预。置换型手术干预研究中的心内膜炎、血栓栓塞和动脉瘤合并发生率较高。16项研究纳入荟萃分析。保留型干预与心内膜炎风险降低相关(RR = 0.13,95%CI:0.03 - 0.61);然而,置换型干预有利于避免瓣膜再次手术(RR = 2.39,95%CI:1.24 - 4.60)。所有研究的偏倚风险均较低。
最佳手术技术的选择取决于疾病类型(MFS或其他结缔组织疾病)以及伴随的主动脉和心血管损伤,因为这些关键因素是异质性的。尽管本荟萃分析的结果倾向于显示一种手术干预相对于另一种手术干预有一些优势,反之亦然,但外科医生只能在手术过程中做出最佳决策。