Leeper Sarah C, Patel Mehul D, Lahri Sa'ad, Beja-Glasser Alexander, Reddy Priscilla, Martin Ian B K, van Hoving Daniël J, Myers Justin G
University of Maryland Medical Center, Emergency Medicine, Cheverly, MD, USA.
University of North Carolina at Chapel Hill School of Medicine, Department of Emergency Medicine, Chapel Hill, NC, USA.
Afr J Emerg Med. 2021 Dec;11(4):379-384. doi: 10.1016/j.afjem.2021.07.001. Epub 2021 Sep 6.
Violence is a major cause of death worldwide among youth. The highest mortality rates from youth violence occur in low and middle-income countries (LMICs). We sought to identify risk factors for violent re-injury and emergency centre (EC) recidivism among assault-injured youth in South Africa.
A prospective follow up study of assault injured youth and controls ages 14-24 presenting for emergency care was conducted in Khayelitsha, South Africa from 2016 to 2018. Sociodemographic and behavioral factors were assessed using a questionnaire administered during the index EC visit. The primary outcomes were return EC visit for violent injury or death within 15 months. We used multivariable logistic regression to compute adjusted odds ratios (OR) and 95% confidence intervals (CI) of associations between return EC visits and key demographic, social, and behavioral factors among assault-injured youth.
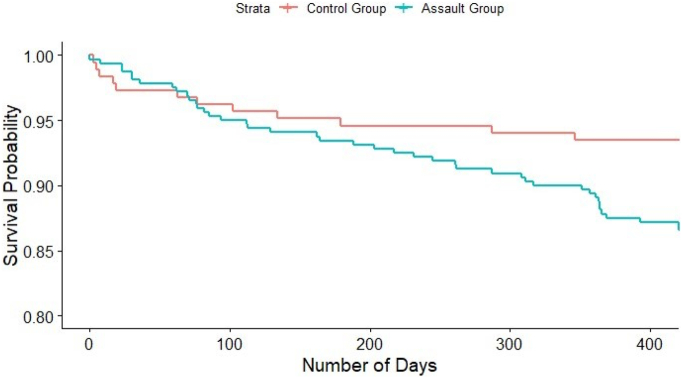
Our study sample included 320 assault-injured patients and 185 non-assault-injured controls. Of the assault-injured, 80% were male, and the mean age was 20.8 years. The assault-injured youth was more likely to have a return EC visit for violent injury (14%) compared to the control group (3%). The non-assault-injured group had a higher mortality rate (7% vs 3%). All deaths in the control group were due to end-stage HIV or TB-related complications. The strongest risk factors for return EC visit were prior criminal activity (OR = 2.3, 95% CI = 1.1-5.1), and current enrollment in school (OR = 2.1, 95% CI = 1.0-4.6). Although the assault-injured group reported high rates of binge drinking (73%) at the index visit, this was not found to be a risk factor for violence-related EC recidivism.
Our findings suggest that assault-injured youth in an LMIC setting are at high risk of EC recidivism and several sociodemographic and behavioral factors are associated with increased risk. These findings can inform targeted intervention programs.
暴力是全球青年死亡的主要原因。青年暴力死亡率最高的地区是低收入和中等收入国家(LMICs)。我们试图确定南非受袭击受伤青年再次遭受暴力伤害和急诊中心(EC)再入院的风险因素。
2016年至2018年在南非开普敦凯伊利沙镇对14至24岁因袭击受伤前来接受急诊治疗的青年及其对照组进行了一项前瞻性随访研究。在首次急诊就诊期间通过问卷调查评估社会人口统计学和行为因素。主要结局是在15个月内因暴力伤害或死亡再次到急诊中心就诊。我们使用多变量逻辑回归计算受袭击受伤青年再次到急诊中心就诊与关键人口统计学、社会和行为因素之间关联的调整比值比(OR)和95%置信区间(CI)。
我们的研究样本包括320名受袭击受伤患者和185名未受袭击受伤的对照组。在受袭击受伤者中,80%为男性,平均年龄为20.8岁。与对照组(3%)相比,受袭击受伤青年因暴力伤害再次到急诊中心就诊的可能性更高(14%)。未受袭击受伤组的死亡率更高(7%对3%)。对照组的所有死亡均归因于晚期艾滋病毒或结核病相关并发症。再次到急诊中心就诊的最强风险因素是既往犯罪活动(OR = 2.3,95% CI = 1.1 - 5.1)和目前在校就读(OR = 2.1,95% CI = 1.0 - 4.6)。尽管受袭击受伤组在首次就诊时报告酗酒率很高(73%),但这并未被发现是与暴力相关的急诊再入院的风险因素。
我们的研究结果表明,低收入和中等收入国家环境中受袭击受伤的青年急诊再入院风险很高,并且一些社会人口统计学和行为因素与风险增加相关。这些发现可为有针对性的干预项目提供参考。