Poostizadeh Ahmad, Jamieson W R Eric, Munro A Ian, Miyagishima Robert T, Ling Hilton, Fradet Guy J, Janusz Michael T, Burr Lawrence H
Department of Surgery, Vancouver Coastal Health Research Institute, University of British Columbia, 2635 (6TH Floor) 2635 Laurel St., Vancouver, BC, V5Z1M9, Canada.
J Cardiothorac Surg. 2021 Sep 16;16(1):262. doi: 10.1186/s13019-021-01631-7.
The prosthesis type for multiple valve surgery (replacement of two or more diseased native or prosthetic valves, replacement of two diseased valves with repair/reconstruction of a third, or replacement of a single diseased valve with repair/reconstruction of a second valve) remains inadequately evaluated. The clinical performance of multiple valve surgery with bioprostheses (BP) and mechanical prostheses (MP) was assessed to compare patient survival and composites of valve-related complications.
Between 1975 and 2000, 1245 patients had multiple valve surgery (BP 785, mean age 62.0 ± 14.7 years; and MP 460, mean age 56.9 ± 12.9 years). There were 1712 procedures performed [BP 969(56.6%) and MP 743(43.4%). Concomitant coronary artery bypass (conCABG) was BP 206(21.3%) and MP 105(14.1%) (p = 0.0002). The cumulative follow-up was BP 5131 years and MP 3364 years. Independent predictors were determined for mortality, valve-related complications and composites of complications.
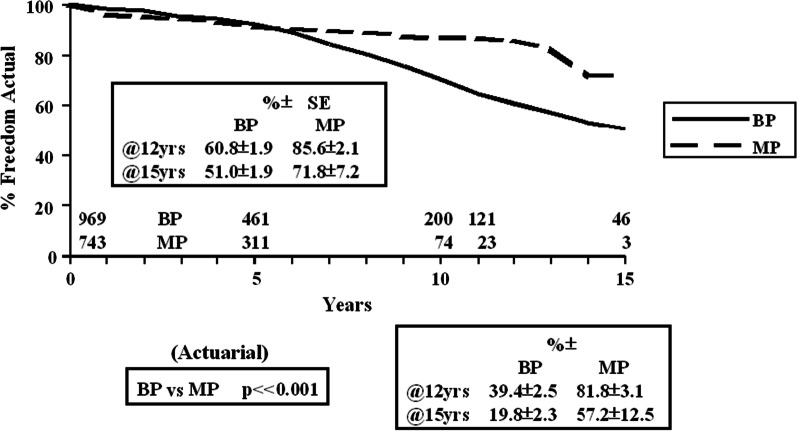
Unadjusted patient survival at 12 years was BP 52.1 ± 2.1% and MP 54.8 ± 4.6% (p = 0.1127), while the age adjusted survival was BP 48.7 ± 2.3% and MP 54.4 ± 5.0%. The predictors of overall mortality were age [Hazard Ratio (HR) 1.051, p < 0.0001], previous valve (HR 1.366, p = 0.028) and conCABG (HR 1.27, p = 0.021). The actual freedom from valve-related mortality at 12 years was BP 85.6 ± 1.6% and MP 91.0 ± 1.6% (actuarial p = 0.0167). The predictors of valve-related mortality were valve type (BP > MP) (2.61, p = 0.001), age (HR 1.032, p = 0.0005) and previous valve (HR 12.61, p < 0.0001). The actual freedom from valve-related reoperation at 12 years was BP 60.8 ± 1.9% and MP85.6 ± 2.1% (actuarial p < 0.001). The predictors of valve-related reoperation were valve type (MP > BP) (HR 0.32, p < 0.0001), age (HR 0.99, p = 0.0001) and previous valve (HR 1.38, p = 0.008) CONCLUSIONS: Overall survival (age adjusted) is differentiated by valve type over 10 and 12 years and valve-related mortality and valve-related reoperation favours the use of mechanical prostheses, overall for multiple valve surgery.
多瓣膜手术(置换两个或更多病变的天然瓣膜或人工瓣膜、置换两个病变瓣膜并修复/重建第三个瓣膜、或置换一个病变瓣膜并修复/重建第二个瓣膜)的假体类型仍未得到充分评估。评估了生物假体(BP)和机械假体(MP)进行多瓣膜手术的临床性能,以比较患者生存率和瓣膜相关并发症的综合情况。
1975年至2000年期间,1245例患者接受了多瓣膜手术(BP组785例,平均年龄62.0±14.7岁;MP组460例,平均年龄56.9±12.9岁)。共进行了1712例手术[BP组969例(56.6%),MP组743例(43.4%)]。同期冠状动脉搭桥术(conCABG)在BP组为206例(21.3%),在MP组为105例(14.1%)(p = 0.0002)。累积随访时间BP组为5131年,MP组为3364年。确定了死亡率、瓣膜相关并发症和并发症综合情况的独立预测因素。
12年时未调整的患者生存率BP组为52.1±2.1%,MP组为54.8±4.6%(p = 0.1127),而年龄调整后的生存率BP组为48.7±2.3%,MP组为54.4±5.0%。总体死亡率的预测因素为年龄[风险比(HR)1.051,p < 0.0001]、既往瓣膜手术史(HR 1.366,p = 0.028)和同期冠状动脉搭桥术(HR 1.27,p = 0.021)。12年时实际无瓣膜相关死亡的比例BP组为85.6±1.6%,MP组为91.0±1.6%(精算p = 0.0167)。瓣膜相关死亡的预测因素为瓣膜类型(BP > MP)(2.61,p = 0.001)、年龄(HR 1.032,p = 0.0005)和既往瓣膜手术史(HR 12.61,p < 0.0001)。12年时实际无瓣膜相关再次手术的比例BP组为60.8±1.9%,MP组为85.6±2.1%(精算p < 0.001)。瓣膜相关再次手术的预测因素为瓣膜类型(MP > BP)(HR 0.32,p < 0.0001)、年龄(HR 0.99,p = 0.0001)和既往瓣膜手术史(HR 1.38,p = 0.008)。结论:总体生存率(年龄调整后)在10年和12年时因瓣膜类型而异,瓣膜相关死亡率和瓣膜相关再次手术倾向于使用机械假体,总体适用于多瓣膜手术。