Irish National Breast Screening Programme and Department of Histopathology, St. Vincent's University Hospital, Elm Park, Dublin 4, Ireland.
School of Medicine, University College Dublin, Dublin, Ireland.
Virchows Arch. 2022 Jan;480(1):177-189. doi: 10.1007/s00428-021-03185-4. Epub 2021 Sep 18.
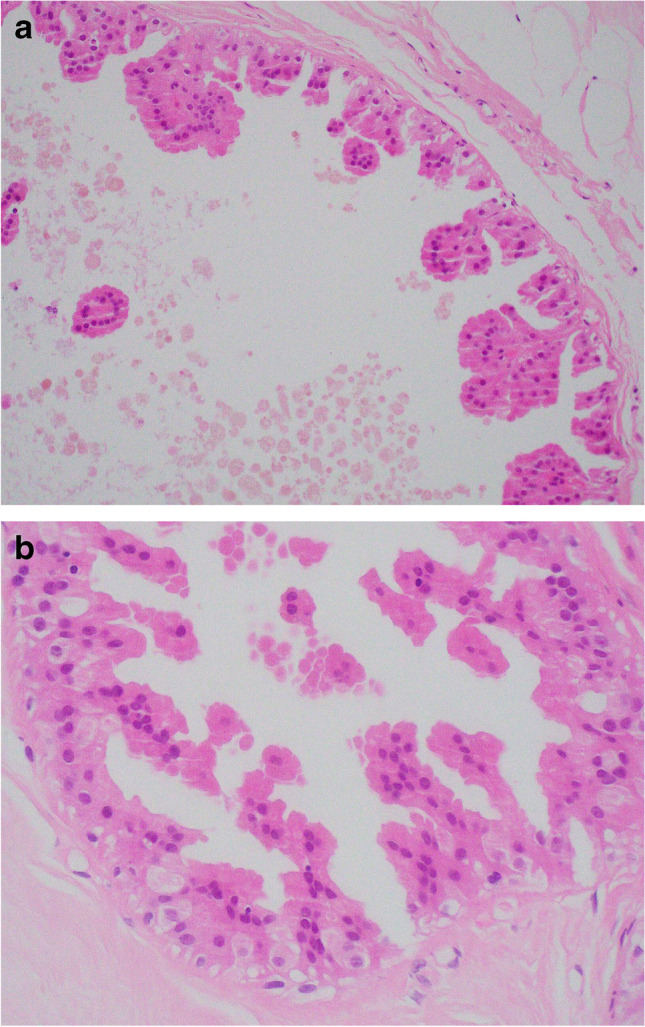
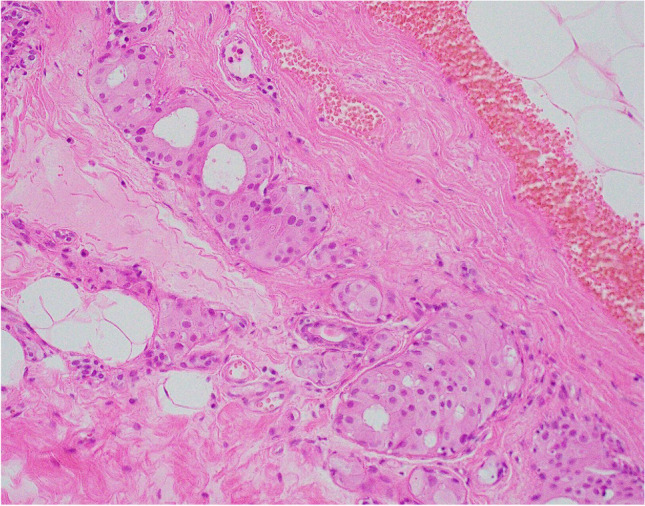
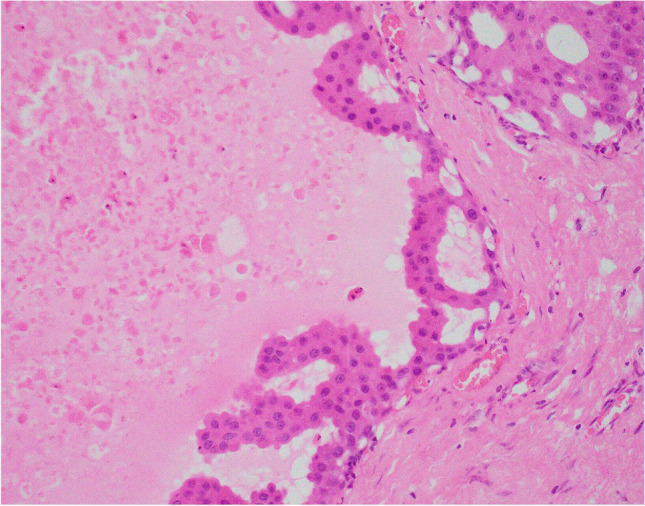
Apocrine change is recognised in benign, atypical and malignant lesions of the breast. Apocrine metaplasia, a frequent finding in the breast of women over the age of 25 years, is most commonly seen in benign cysts with a simple or papillary configuration. Apocrine change is also recognised in other benign lesions including sclerosing adenosis, now known as apocrine adenosis. Apocrine atypia usually refers to cytological atypia in which there is at least threefold variation in nuclear size but architectural atypia may also occur. The distinction between atypical apocrine hyperplasia and non-high-grade apocrine ductal carcinoma in situ may be difficult due to the relative rarity of these entities and the lack of validated diagnostic criteria. Lobular carcinoma in situ (LCIS) with apocrine change is considered to be a variant of pleomorphic LCIS. An apocrine variant of encapsulated papillary carcinoma is also recognised. Apocrine change is described in invasive carcinoma, including no special type, lobular, micropapillary and mucinous variants. The recent WHO 2019 update recognises 'carcinoma with apocrine differentiation' as a special type breast carcinoma based on the presence of apocrine morphology in at least 90% of the tumour. Tumours with apocrine morphology are usually but not always hormone receptor negative. Human epidermal growth factor receptor 2 (HER-2) status is variable. Molecular studies have identified breast tumours with apocrine features and high expression of androgen receptor mRNA including 'luminal androgen receptor tumours' and 'molecular apocrine tumours'. The term 'pure apocrine carcinoma' has been proposed to describe an invasive carcinoma with apocrine morphology that is oestrogen and progesterone receptor negative and androgen receptor positive. HER-2 status may be positive or negative. This article reviews the pathology of benign, atypical and malignant apocrine lesions of the breast, with emphasis on diagnostic criteria including an approach to evaluation of apocrine lesions on needle core biopsy, and recent advances in our understanding of invasive apocrine carcinoma.
大汗腺化生可见于乳腺的良性、非典型和恶性病变。大汗腺化生是一种常见于 25 岁以上女性乳腺的病变,最常发生于单纯性或乳头状结构的良性囊肿中。大汗腺化生也可见于其他良性病变,包括硬化性腺病,现称为大汗腺性腺病。大汗腺非典型性通常是指细胞学非典型性,其中核大小至少有三倍的变化,但也可能发生结构非典型性。由于这些病变相对罕见,且缺乏经过验证的诊断标准,因此非典型大汗腺增生与非高级别大汗腺导管原位癌之间的鉴别可能较为困难。伴有大汗腺化生的乳腺小叶原位癌(LCIS)被认为是多形性 LCIS 的一种变异型。也认识到包裹性乳头状癌的大汗腺变异型。大汗腺化生可见于浸润性癌,包括非特殊型、小叶型、微乳头状和黏液型变体。最近的 2019 年 WHO 更新将“具有大汗腺分化的癌”确认为一种特殊类型的乳腺癌,基于至少 90%的肿瘤存在大汗腺形态。具有大汗腺形态的肿瘤通常但并非总是激素受体阴性。人表皮生长因子受体 2(HER-2)状态是可变的。分子研究已经确定了具有大汗腺特征和雄激素受体 mRNA 高表达的乳腺肿瘤,包括“腔内分泌型雄激素受体肿瘤”和“分子型大汗腺肿瘤”。提出“纯大汗腺癌”一词来描述一种具有大汗腺形态的浸润性癌,雌激素和孕激素受体阴性,雄激素受体阳性。HER-2 状态可能是阳性或阴性。本文回顾了乳腺良性、非典型和恶性大汗腺病变的病理学,重点介绍了诊断标准,包括对针芯活检中大汗腺病变的评估方法,以及对浸润性大汗腺癌认识的最新进展。