Paediatric Neurology and Neurophysiology Unit, Department of Women's and Children's Health, University Hospital of Padova, Padova, Italy.
Neuroimmunology Group, Paediatric Research Institute "Città della Speranza," Padova, Italy.
JAMA Neurol. 2021 Nov 1;78(11):1333-1344. doi: 10.1001/jamaneurol.2021.3188.
Overall, immunotherapy has been shown to improve outcomes and reduce relapses in individuals with N-methyl-d-aspartate receptor (NMDAR) antibody encephalitis (NMDARE); however, the superiority of specific treatments and combinations remains unclear.
To map the use and safety of immunotherapies in individuals with NMDARE, identify early predictors of poor functional outcome and relapse, evaluate changes in immunotherapy use and disease outcome over the 14 years since first reports of NMDARE, and assess the Anti-NMDAR Encephalitis One-Year Functional Status (NEOS) score.
Systematic search in PubMed from inception to January 1, 2019.
Published articles including patients with NMDARE with positive NMDAR antibodies and available individual immunotherapy data.
Individual patient data on immunotherapies, clinical characteristics at presentation, disease course, and final functional outcome (modified Rankin Scale [mRS] score) were entered into multivariable logistic regression models.
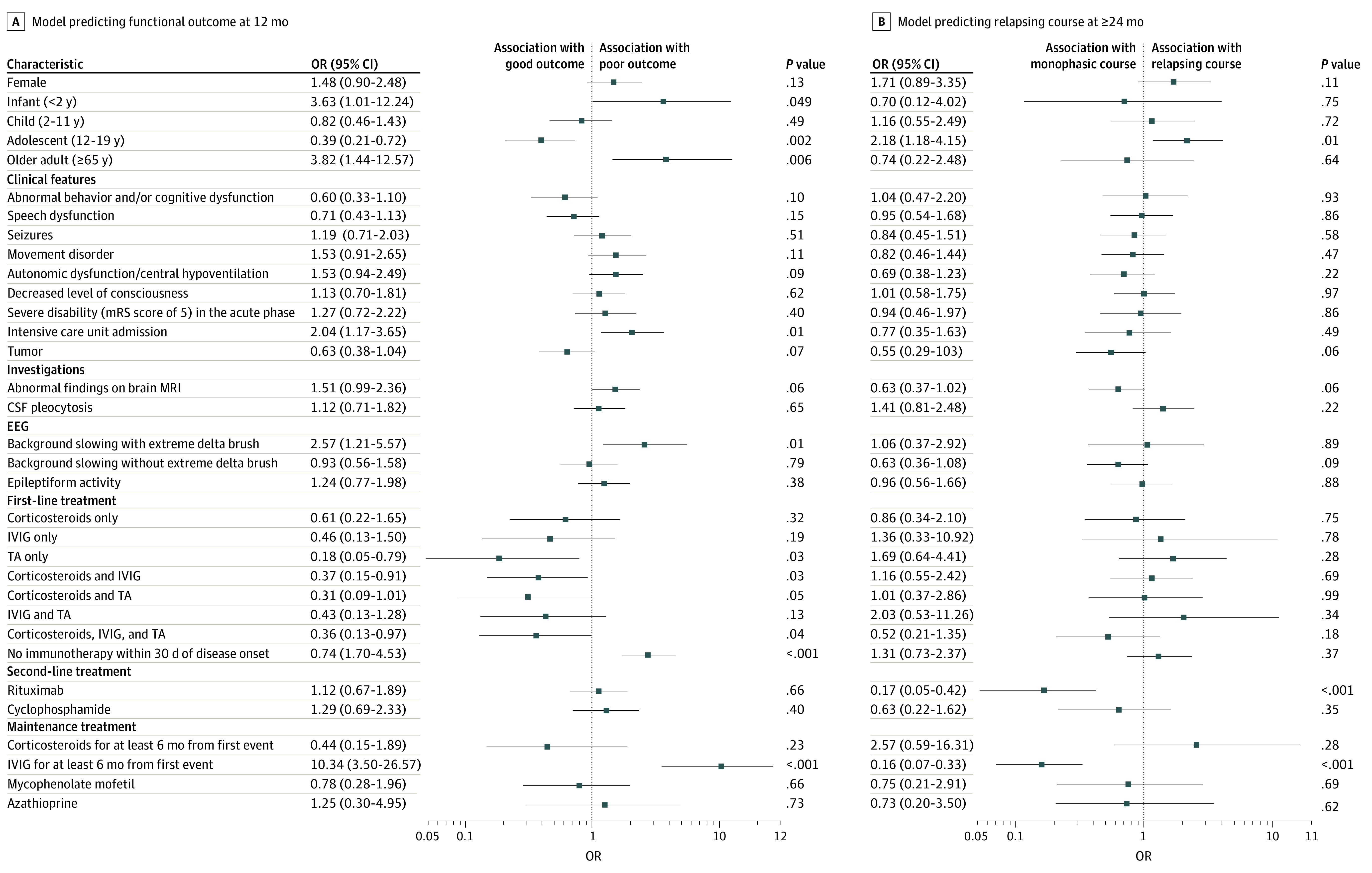
The planned study outcomes were functional outcome at 12 months from disease onset (good, mRS score of 0 to 2; poor, mRS score greater than 2) and monophasic course (absence of relapse at 24 months or later from onset).
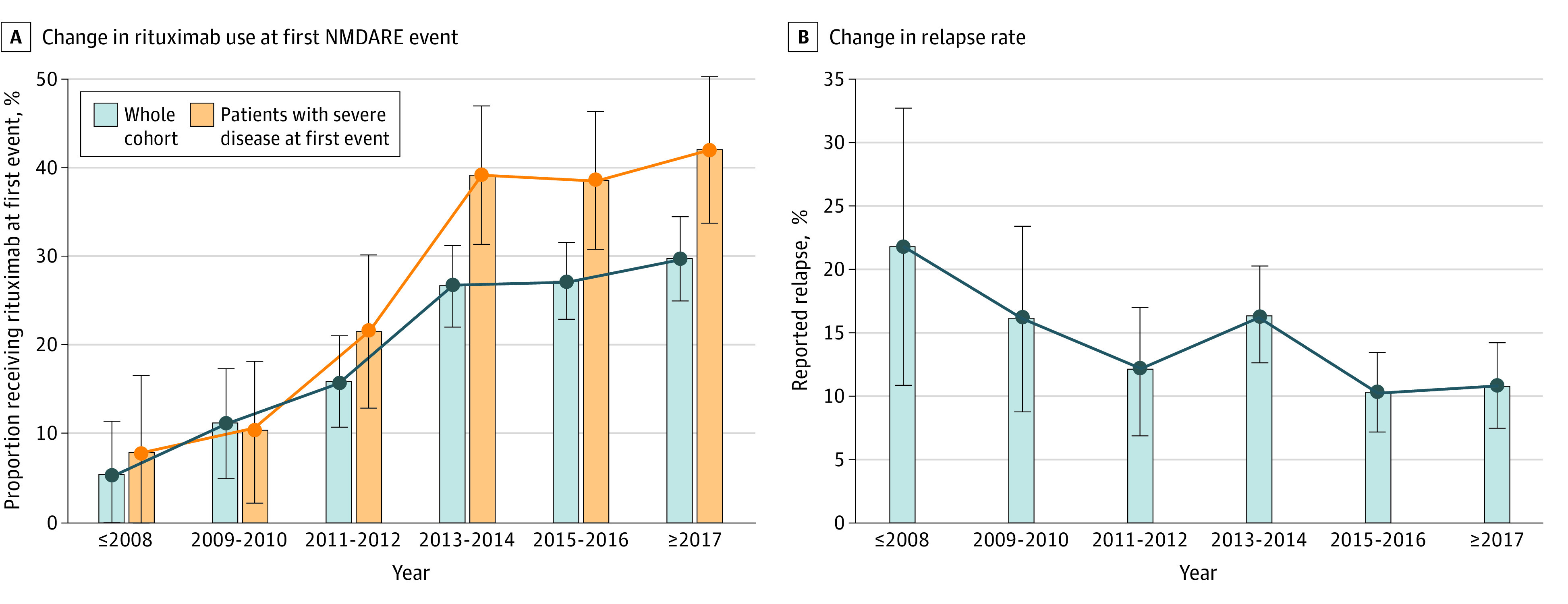
Data from 1550 patients from 652 articles were evaluated. Of these, 1105 of 1508 (73.3%) were female and 707 of 1526 (46.3%) were 18 years or younger at disease onset. Factors at first event that were significantly associated with good functional outcome included adolescent age and first-line treatment with therapeutic apheresis, corticosteroids plus intravenous immunoglobulin (IVIG), or corticosteroids plus IVIG plus therapeutic apheresis. Factors significantly associated with poor functional outcome were age younger than 2 years or age of 65 years or older at onset, intensive care unit admission, extreme delta brush pattern on electroencephalography, lack of immunotherapy within the first 30 days of onset, and maintenance IVIG use for 6 months or more. Factors significantly associated with nonrelapsing disease were rituximab use or maintenance IVIG use for 6 months or more. Adolescent age at onset was significantly associated with relapsing disease. Rituximab use increased from 13.5% (52 of 384; 2007 to 2013) to 28.3% (311 of 1100; 2013 to 2019) (P < .001), concurrent with a falling relapse rate over the same period (22% [12 of 55] in 2008 and earlier; 10.9% [35 of 322] in 2017 and later; P = .006). Modified NEOS score (including 4 of 5 original NEOS items) was associated with probability of poor functional status at 1 year (20.1% [40 of 199] for a score of 0 to 1 points; 43.8% [77 of 176] for a score of 3 to 4 points; P = .05).
Factors influencing functional outcomes and relapse are different and need to be considered independently in development of evidence-based optimal management guidelines of patients with NMDARE.
总的来说,免疫疗法已被证明可以改善 N-甲基-D-天冬氨酸受体 (NMDAR) 抗体脑炎 (NMDARE) 患者的预后并减少复发;然而,具体治疗方法和联合治疗的优势仍不清楚。
绘制 NMDARE 患者免疫治疗的使用和安全性图谱,确定不良功能结局和复发的早期预测因素,评估自首次报道 NMDARE 以来 14 年间免疫治疗使用和疾病结局的变化,并评估抗 NMDAR 脑炎一年功能状态 (NEOS) 评分。
从开始到 2019 年 1 月 1 日在 PubMed 进行系统搜索。
发表的文章包括 NMDARE 患者,其 NMDAR 抗体呈阳性,且有可用的个体免疫治疗数据。
将免疫治疗、发病时的临床特征、疾病过程和最终功能结局(改良 Rankin 量表 [mRS] 评分)的个体患者数据输入多变量逻辑回归模型。
计划的研究结局是疾病发病后 12 个月的功能结局(良好,mRS 评分为 0 至 2;不良,mRS 评分大于 2)和单相病程(发病后 24 个月或之后无复发)。
对来自 652 篇文章的 1550 名患者的数据进行了评估。其中,1508 名患者中有 1105 名(73.3%)为女性,1526 名患者中有 707 名(46.3%)在发病时为 18 岁或以下。首次发病时与良好功能结局相关的因素包括青少年年龄和一线治疗方法为血浆置换、皮质类固醇加静脉免疫球蛋白 (IVIG) 或皮质类固醇加 IVIG 加血浆置换。与不良功能结局显著相关的因素包括发病时年龄小于 2 岁或年龄大于 65 岁、入住重症监护病房、脑电图出现极度德尔塔刷样模式、发病后 30 天内未进行免疫治疗以及维持性 IVIG 使用 6 个月或更长时间。与非复发疾病显著相关的因素包括使用利妥昔单抗或维持性 IVIG 使用 6 个月或更长时间。发病时的青少年年龄与复发疾病显著相关。利妥昔单抗的使用从 2007 年至 2013 年的 13.5%(52/384)增加到 2013 年至 2019 年的 28.3%(311/1100)(P < .001),同时在此期间复发率下降(2008 年及之前为 22%[12/55];2017 年及之后为 10.9%[35/322];P = .006)。改良后的 NEOS 评分(包括原始 NEOS 项目中的 4 项)与 1 年后不良功能状态的概率相关(评分 0 至 1 分的为 20.1%[40/199];评分 3 至 4 分的为 43.8%[77/176];P = .05)。
影响功能结局和复发的因素不同,在制定 NMDARE 患者的循证最佳管理指南时需要单独考虑。