Université de Lorraine, Centre d'Investigations Cliniques Plurithématique 1433 and Inserm U1116, Centre Hospitalier Universitaire de Nancy, FCRIN INI-CRCT (Cardiovascular and Renal Clinical Trialists), Nancy, France.
Cardiovascular Research and Development Center, Department of Surgery and Physiology, Faculty of Medicine of the University of Porto, Porto, Portugal.
Diabetes Obes Metab. 2022 Jan;24(1):135-141. doi: 10.1111/dom.14559. Epub 2021 Oct 4.
To evaluate the effect of empagliflozin on uric acid (UA) levels, antigout medication and gout episodes in the EMPA-REG OUTCOME trial (NCT01131676).
A total of 7020 patients with type 2 diabetes (T2D) were randomized to either empagliflozin (10 or 25 mg) or placebo. The effects of empagliflozin versus placebo on UA concentration were assessed using mixed linear models. A composite outcome of new prescription of antigout medication or gout episode was studied with Cox proportional hazards models.
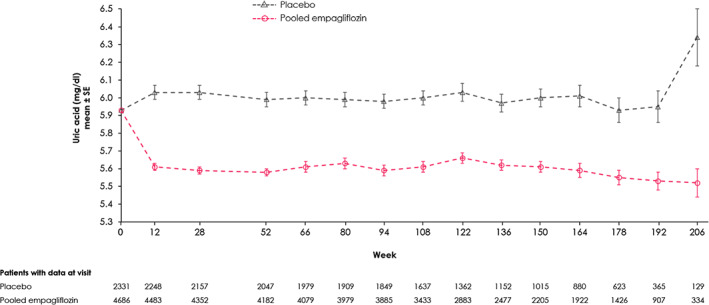
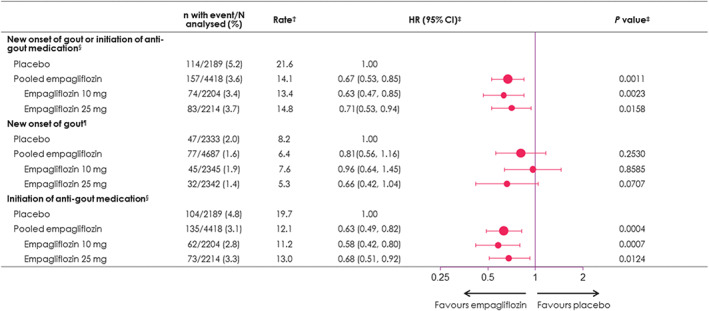
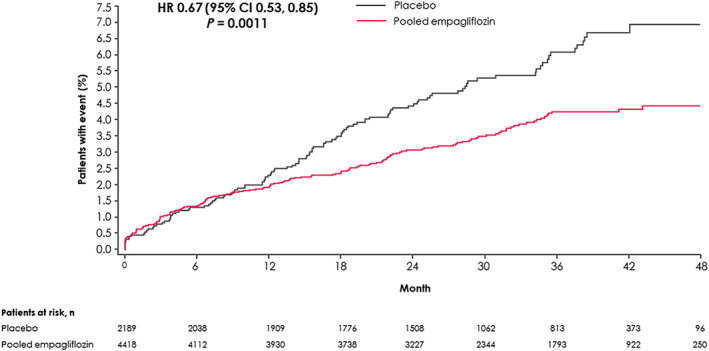
Empagliflozin reduced serum UA levels versus placebo: week 52 adjusted mean treatment difference = -0.37 (95% confidence interval [CI] -0.42, -0.31) mg/dL; this was more pronounced in patients with baseline UA ≥ 7.0 mg/dL versus <7.0 mg/dL: week 52 adjusted mean treatment difference = -0.56 (95% CI -0.68, -0.43) and -0.30 (95% CI -0.37, -0.24) mg/dL, respectively. Among 6607 patients not taking antigout medications at baseline, 5.2% had a gout episode or initiated antigout treatment versus 3.6% in the placebo and empagliflozin groups, respectively: hazard ratio 0.67 (95% CI 0.53, 0.85; P = 0.001). Both components of the composite outcome contributed to the reduction with empagliflozin in the composite. Risk reduction was similar with both empagliflozin doses.
Empagliflozin reduced UA levels and the composite of gout episodes or prescription of antigout medication. These clinically important findings expand the utility of empagliflozin as a potential antigout treatment in patients with T2D, beyond its well-established cardio-renal benefits.
评估恩格列净对 EM-PA-REG OUTCOME 试验(NCT01131676)中尿酸(UA)水平、抗痛风药物和痛风发作的影响。
7020 例 2 型糖尿病(T2D)患者被随机分为恩格列净(10 或 25mg)或安慰剂组。采用混合线性模型评估恩格列净与安慰剂对 UA 浓度的影响。采用 Cox 比例风险模型研究新处方抗痛风药物或痛风发作的复合结局。
与安慰剂相比,恩格列净降低了血清 UA 水平:第 52 周调整后的平均治疗差异为-0.37(95%置信区间[CI] -0.42,-0.31)mg/dL;在基线 UA≥7.0mg/dL的患者中更为明显,与<7.0mg/dL的患者相比:第 52 周调整后的平均治疗差异为-0.56(95% CI -0.68,-0.43)和-0.30(95% CI -0.37,-0.24)mg/dL。在 6607 例基线时未服用抗痛风药物的患者中,有 5.2%发生痛风发作或开始使用抗痛风药物,而安慰剂和恩格列净组分别为 3.6%:风险比 0.67(95% CI 0.53,0.85;P=0.001)。复合结局的两个组成部分均有助于降低恩格列净治疗组的复合结局。两种剂量的恩格列净的风险降低相似。
恩格列净降低了 UA 水平和痛风发作或处方抗痛风药物的复合结局。这些具有临床重要意义的发现扩大了恩格列净作为 2 型糖尿病潜在抗痛风治疗的应用范围,超出了其已确立的心脏肾脏获益。