Li SiNi, Li JianHe, Peng LiuBao, Li YaMin, Wan XiaoMin
Clinical Nursing Teaching and Research Section, The Second Xiangya Hospital, Central South University, Changsha, China.
The Xiangya Nursing School, Central South University, Changsha, China.
Front Pharmacol. 2021 Sep 9;12:718014. doi: 10.3389/fphar.2021.718014. eCollection 2021.
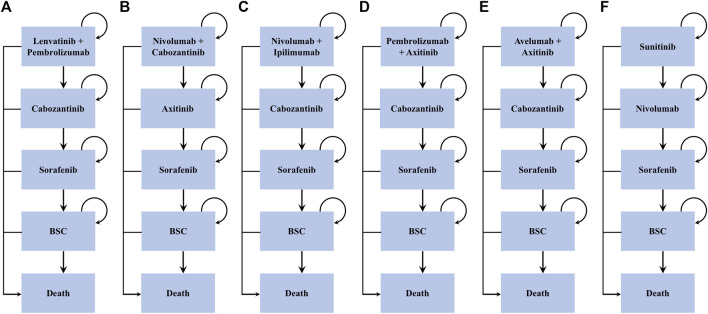
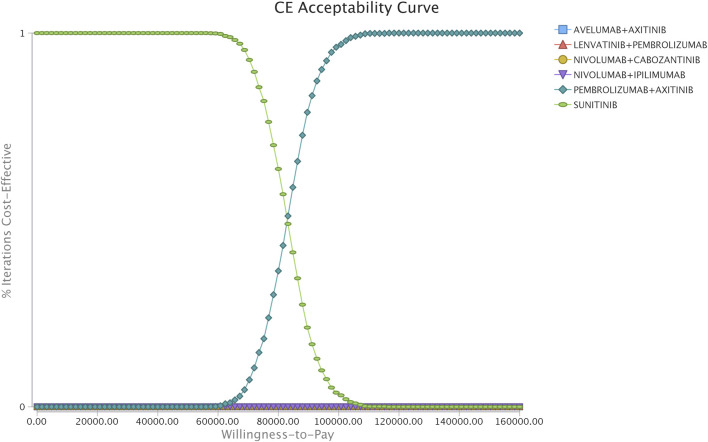
Recent randomized controlled trials have demonstrated that immune checkpoint inhibitors (ICIs) improve patient outcomes, but whether these novel agents are cost-effective for untreated advanced renal cell carcinoma (aRCC) remains unclear. A microsimulation model was created to project the healthcare costs and outcomes of six strategies (lenvatinib-plus-pembrolizumab, nivolumab-plus-cabozantinib, nivolumab-plus-ipilimumab, pembrolizumab-plus-axitinib, avelumab-plus-axitinib, and sunitinib monotherapy) for patients with aRCC. Transition probability of patients was estimated from CLEAR, CheckMate 9ER, CheckMate 214, KEYNOTE-426, JAVELIN Renal 101, and other data sets by using parametric survival modeling. Lifetime direct medical costs, life years (LYs), quality-adjusted LYs (QALYs), and incremental cost-effectiveness ratios (ICERs) were estimated from a United States payer perspective. One-way and probabilistic sensitivity analyses were performed, along with multiple scenario analyses, to evaluate model uncertainty. Of the six competing strategies, nivolumab-plus-cabozantinib yielded the most significant health outcomes, and the sunitinib strategy was the least expensive option. The cost-effective frontier consisted of the nivolumab-plus-cabozantinib, pembrolizumab-plus-axitinib, and sunitinib strategies, which displayed the ordered ICERs of $81282/QALY for pembrolizumab-plus-axitinib vs sunitinib and $453391/QALY for nivolumab-plus-cabozantinib vs pembrolizumab-plus-axitinib. The rest of the strategies, such as lenvatinib-plus-pembrolizumab, nivolumab-plus-ipilimumab, and avelumab-plus-axitinib, were dominated. The cost of sunitinib drove the model most influentially. For aRCC, the pembrolizumab-plus-axitinib strategy is likely to be the most cost-effective alternative at the willingness-to-pay threshold of $100,000.
近期的随机对照试验表明,免疫检查点抑制剂(ICIs)可改善患者预后,但这些新型药物对于未经治疗的晚期肾细胞癌(aRCC)是否具有成本效益仍不明确。创建了一个微观模拟模型,以预测aRCC患者六种治疗策略(乐伐替尼联合帕博利珠单抗、纳武利尤单抗联合卡博替尼、纳武利尤单抗联合伊匹木单抗、帕博利珠单抗联合阿昔替尼、阿维鲁单抗联合阿昔替尼以及舒尼替尼单药治疗)的医疗成本和预后。通过使用参数生存模型,根据CLEAR、CheckMate 9ER、CheckMate 214、KEYNOTE - 426、JAVELIN Renal 101及其他数据集估算患者的转移概率。从美国医保支付方的角度估算终身直接医疗成本、生命年(LYs)、质量调整生命年(QALYs)以及增量成本效益比(ICERs)。进行了单因素和概率敏感性分析以及多种情景分析,以评估模型的不确定性。在这六种竞争策略中,纳武利尤单抗联合卡博替尼产生的健康效益最为显著,舒尼替尼策略是成本最低的选择。成本效益前沿包括纳武利尤单抗联合卡博替尼、帕博利珠单抗联合阿昔替尼以及舒尼替尼策略,帕博利珠单抗联合阿昔替尼相对于舒尼替尼的ICER为81282美元/QALY,纳武利尤单抗联合卡博替尼相对于帕博利珠单抗联合阿昔替尼的ICER为453391美元/QALY。其余策略,如乐伐替尼联合帕博利珠单抗、纳武利尤单抗联合伊匹木单抗以及阿维鲁单抗联合阿昔替尼,则处于劣势。舒尼替尼的成本对模型的影响最为显著。对于aRCC,在支付意愿阈值为100,000美元时,帕博利珠单抗联合阿昔替尼策略可能是最具成本效益的选择。