Panda Prashant, Singh Neena Vir, Kaur Navjyot, Kaur Prabhjot, Kaur Avneet, Aujla Harleen Kaur, Kaur Khushpreet, Saini Nishtha, Kapoor Shakshi, Paul Sharma Yash
Cardiology, Postgraduate Institute of Medical Education & Research, Chandigarh, IND.
Nursing, National Institute of Nursing Education, Postgraduate Institute of Medical Education & Research, Chandigarh, IND.
Cureus. 2021 Aug 22;13(8):e17369. doi: 10.7759/cureus.17369. eCollection 2021 Aug.
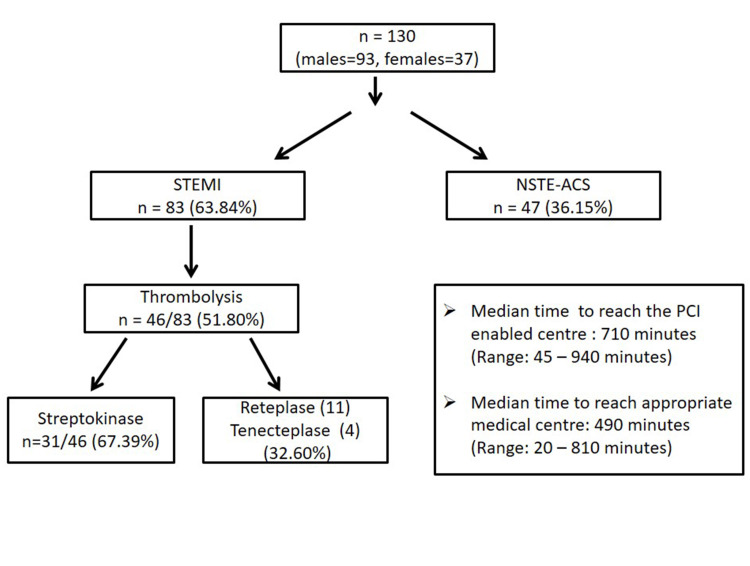
Background Various Indian registries have documented a delay of more than five hours for acute coronary syndrome patients from onset of symptoms to reaching thrombolysis-enabled centres. We conducted this study to evaluate the factors responsible for pre-hospital delay in acute coronary syndrome patients. Methods This was a descriptive cross-sectional study conducted in consecutive acute coronary syndrome patients who reported to the tertiary care medical centre in North India. A standardized tool was used to record the demographic data, socioeconomic status and clinical presentation of patients. All factors which led to pre-hospital delay were noted and the appropriate statistical tests were used for analysis. Results A total of 130 patients (males=93, females=37) were included in the study. The median time at which the acute coronary syndrome patients presented to the thrombolysis and percutaneous coronary intervention enabled centre was 490 minutes (range: 20 - 810 minutes) and 710 minutes (range: 45 - 940 minutes) respectively. The various factors responsible for prehospital delay were rural residence (p-value <0.0001), visit to local dispensary (p-value=0.0023), delay in getting transport (p-value=0.03) and misinterpretation of cardiac symptoms (p-value=0.0004). A significant but weak negative correlation was found between per capita income, decision making time and time taken to receive thrombolytic therapy. Out of a total of 83 ST-elevation myocardial infarction patients, only 46 (51.80%) were thrombolysed. Though 69/83 (83.13%) ST-elevation myocardial infarction patients reached thrombolysis enabled centre directly, only nine (10.84%) were thrombolysed at first medical contact; the rest were transferred to the percutaneous coronary intervention-enabled centre without any prior information. Conclusion Our study concludes that besides socioeconomic and demographic variables, lack of public awareness, well established public transport & health insurance system lead to significant pre-hospital delays and increase the time to revascularization. Besides, judgemental error on the part of medical practitioners in the peripheries also significantly delays thrombolysis in ST-elevation myocardial infarction patients.
印度的多个登记处记录显示,急性冠状动脉综合征患者从症状发作到抵达具备溶栓能力的中心存在超过5小时的延迟。我们开展这项研究以评估导致急性冠状动脉综合征患者院前延迟的因素。方法:这是一项描述性横断面研究,研究对象为连续就诊于印度北部三级医疗中心的急性冠状动脉综合征患者。使用标准化工具记录患者的人口统计学数据、社会经济状况和临床表现。记录所有导致院前延迟的因素,并使用适当的统计检验进行分析。结果:共有130例患者(男性93例,女性37例)纳入研究。急性冠状动脉综合征患者到达具备溶栓和经皮冠状动脉介入治疗能力中心的中位时间分别为490分钟(范围:20 - 810分钟)和710分钟(范围:45 - 940分钟)。导致院前延迟的各种因素包括农村居住(p值<0.0001)、前往当地药房就诊(p值=0.0023)、获取交通工具延迟(p值=0.03)以及对心脏症状的误解(p值=0.0004)。发现人均收入、决策时间与接受溶栓治疗所需时间之间存在显著但较弱的负相关。在总共83例ST段抬高型心肌梗死患者中,仅46例(51.80%)接受了溶栓治疗。尽管83例ST段抬高型心肌梗死患者中有69例(83.13%)直接到达了具备溶栓能力的中心,但只有9例(10.84%)在首次医疗接触时接受了溶栓治疗;其余患者在没有任何预先通知的情况下被转至具备经皮冠状动脉介入治疗能力的中心。结论:我们的研究得出结论,除了社会经济和人口统计学变量外,公众意识缺乏、完善的公共交通和医疗保险系统导致了显著的院前延迟,并增加了血管再通时间。此外,基层医疗从业者的判断失误也显著延迟了ST段抬高型心肌梗死患者的溶栓治疗。