Katz Austen D, Galina Jesse, Song Junho, Hasan Sayyida, Perfetti Dean, Virk Sohrab, Silber Jeff, Essig David
Department of Orthopedic Surgery, North Shore University Hospital-Long Island Jewish Medical Center, Zucker School of Medicine at Hofstra University, New Hyde Park, NY, USA.
Global Spine J. 2023 Sep;13(7):1728-1736. doi: 10.1177/21925682211047551. Epub 2021 Sep 25.
Retrospective database study.
Navigation has been increasingly used to treat degenerative disease, with positive radiographic and clinical outcomes and fewer adverse events and reoperations, despite increased operative time. However, short-term analysis on treating adult spinal deformity (ASD) surgery with navigation is limited, particularly using large nationally represented cohorts. This is the first large-scale database study to compare 30-day readmission, reoperation, morbidity, and value-per-operative time for navigated and conventional ASD surgery.
Adults were identified in the National Surgical Quality Improvement Program (NSQIP) database. Multivariate regression was used to compare outcomes between navigated and conventional surgery and to control for predictors and baseline differences.
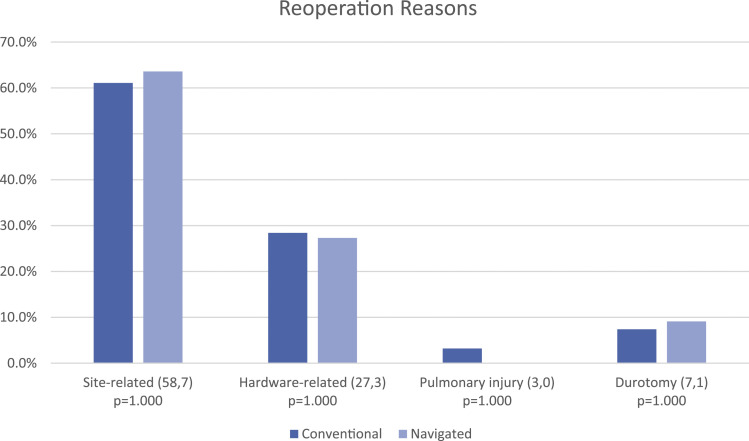
3190 ASD patients were included. Navigated and conventional patients were similar. Navigated cases had greater operative time (405 vs 320 min) and mean RVUs per case (81.3 vs 69.7), and had more supplementary pelvic fixations (26.1 vs 13.4%) and osteotomies (50.3 vs 27.7%) ( <.001).In univariate analysis, navigation had greater reoperation (9.9 vs 5.2%, = .011), morbidity (57.8 vs 46.8%, = .007), and transfusion (52.2 vs 41.8%, = .010) rates. Readmission was similar (11.9 vs 8.4%). In multivariate analysis, navigation predicted reoperation (OR = 1.792, = .048), but no longer predicted morbidity or transfusion. Most reoperations were infectious and hardware-related.
Despite controlling for patient-related and procedural factors, navigation independently predicted a 79% increased odds of reoperation but did not predict morbidity or transfusion. Readmission was similar between groups. This is explained, in part, by greater operative time and transfusion, which are risk factors for infection. Reoperation most frequently occurred for wound- and hardware-related reasons, suggesting navigation carries an increased risk of infectious-related events beyond increased operative time.
回顾性数据库研究。
导航技术已越来越多地用于治疗退行性疾病,尽管手术时间增加,但影像学和临床结果良好,不良事件和再次手术较少。然而,关于导航技术治疗成人脊柱畸形(ASD)手术的短期分析有限,特别是使用具有全国代表性的大型队列研究。这是第一项大规模数据库研究,旨在比较导航ASD手术和传统ASD手术的30天再入院率、再次手术率、发病率以及每手术时间的价值。
在国家外科质量改进计划(NSQIP)数据库中识别成年患者。采用多变量回归分析比较导航手术和传统手术的结果,并控制预测因素和基线差异。
纳入3190例ASD患者。导航组和传统组患者情况相似。导航组手术时间更长(405分钟对320分钟),每例平均相对价值单位(RVUs)更高(81.3对69.7),且更多采用辅助骨盆固定(26.1%对13.4%)和截骨术(50.3%对27.7%)(P<.001)。单变量分析中,导航组再次手术率更高(9.9%对5.2%,P =.011)、发病率更高(57.8%对46.8%,P =.007)和输血率更高(52.2%对41.8%,P =.010)。再入院率相似(11.9%对8.4%)。多变量分析中,导航技术可预测再次手术(OR = 1.792,P =.048),但不再预测发病率或输血情况。大多数再次手术与感染和硬件相关。
尽管控制了患者相关因素和手术相关因素,但导航技术独立预测再次手术的几率增加79%,但不能预测发病率或输血情况。两组再入院率相似。部分原因是手术时间更长和输血更多,这是感染的危险因素。再次手术最常见的原因是伤口和硬件相关,这表明导航技术除了增加手术时间外,还增加了感染相关事件的风险。