Division of Thoracic Oncology, Shizuoka Cancer Center, Shizuoka, Japan.
Department of Biostatistics, Clinical Research Center, Shizuoka Cancer Center, Shizuoka, Japan.
Cancer Med. 2021 Nov;10(21):7503-7513. doi: 10.1002/cam4.4268. Epub 2021 Sep 29.
Epidermal growth factor receptor tyrosine kinase inhibitors (EGFR-TKIs) are currently the primary treatment option for patients with EGFR-mutant non-small cell lung cancer (NSCLC). However, the effect of EGFR-TKIs are eventually weakened due to resistance, and there is also a differential efficacy based on EGFR mutation subtypes. The combination of angiogenesis inhibitor (AI) with EGFR-TKI has shown better efficacy than EGFR-TKI monotherapy, regardless of the mutation subtypes. Nevertheless, the effect of AI eligibility on overall survival (OS) and progression-free survival (PFS) remains to be elucidated. Thus, we assessed this impact on patients with NSCLC harboring EGFR mutation.
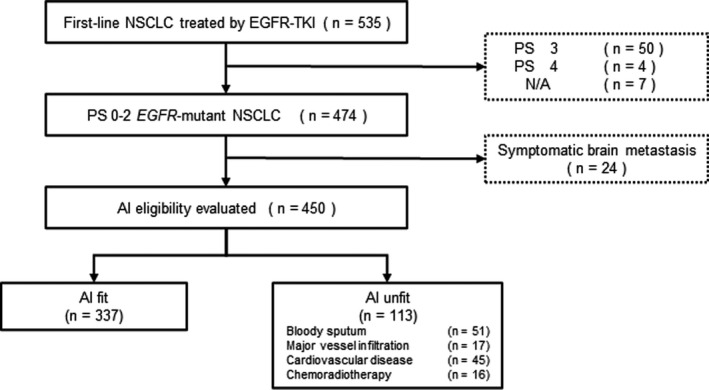
In this study, the data for 450 patients with EGFR-mutant NSCLC, who were treated with EGFR-TKI monotherapy, were retrospectively analyzed for AI eligibility. The patients were categorized into AI-eligible (AI fit) and ineligible groups (AI unfit).
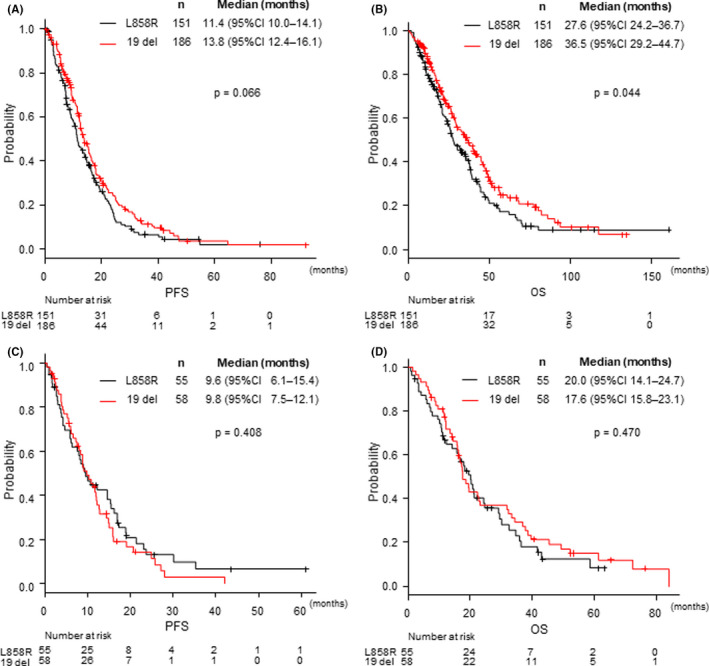
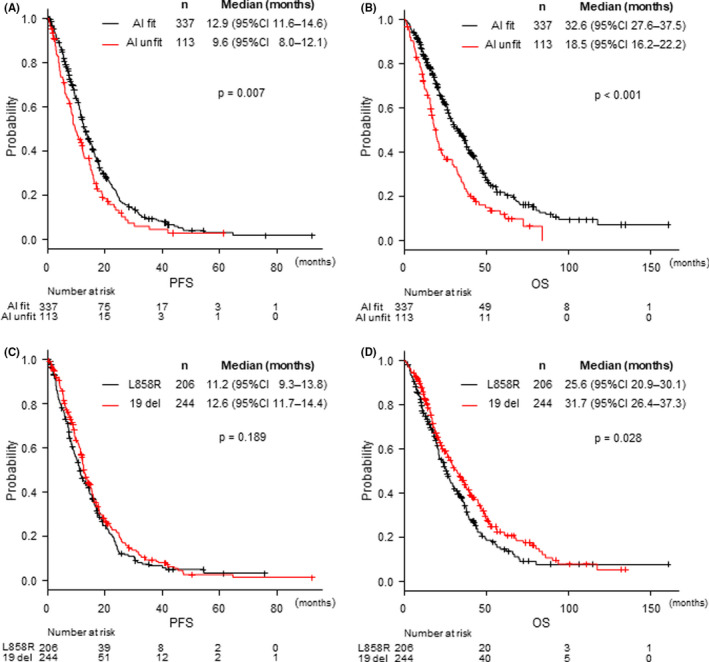
The median PFS of the AI fit group was 12.9 months, compared to 9.6 months in the unfit group (p = 0.007), and OS was also significantly longer in the AI fit group (median OS = 33.0 months) compared to that in the unfit group (18.5 months, p < 0.001). Multivariate analysis indicated that AI ineligibility was associated with shorter PFS and poor prognosis. Also, in the AI fit group, there was no significant difference in the PFS between EGFR L858R mutation and EGFR exon 19 deletion (median PFS = 11.5 months vs. 13.8 months; p = 0.17).
From our study, AI eligibility resulted in longer OS and PFS, and also had different effects on patients with EGFR L858R and exon 19 deletion. Since this selection bias may have affected previous clinical trial data on the efficacy of AI combination therapy, their results should be carefully considered henceforth.
表皮生长因子受体酪氨酸激酶抑制剂(EGFR-TKIs)是目前 EGFR 突变型非小细胞肺癌(NSCLC)患者的主要治疗选择。然而,由于耐药性的出现,EGFR-TKIs 的疗效最终会减弱,并且根据 EGFR 突变亚型的不同,疗效也存在差异。血管生成抑制剂(AI)与 EGFR-TKI 的联合应用显示出比 EGFR-TKI 单药治疗更好的疗效,无论突变亚型如何。然而,AI 资格对总生存期(OS)和无进展生存期(PFS)的影响仍需阐明。因此,我们评估了这对 EGFR 突变的 NSCLC 患者的影响。
本研究回顾性分析了 450 例接受 EGFR-TKI 单药治疗的 EGFR 突变型 NSCLC 患者的 AI 资格数据。患者被分为 AI 合格(AI 适合)和不合格组(AI 不适合)。
AI 适合组的中位 PFS 为 12.9 个月,而不适合组为 9.6 个月(p=0.007),AI 适合组的 OS 也明显长于不适合组(中位 OS=33.0 个月)(p<0.001)。多变量分析表明,AI 不合格与较短的 PFS 和较差的预后相关。此外,在 AI 适合组中,EGFR L858R 突变和 EGFR 外显子 19 缺失患者的 PFS 无显著差异(中位 PFS=11.5 个月比 13.8 个月;p=0.17)。
从我们的研究中可以看出,AI 合格可延长 OS 和 PFS,并且对 EGFR L858R 和外显子 19 缺失患者有不同的影响。由于这种选择偏差可能影响了 AI 联合治疗疗效的先前临床试验数据,因此应谨慎考虑其结果。