Mansfield Aaron S, Herbst Roy S, de Castro Gilberto, Hui Rina, Peled Nir, Kim Dong-Wan, Novello Silvia, Satouchi Miyako, Wu Yi-Long, Garon Edward B, Reck Martin, Robinson Andrew G, Samkari Ayman, Piperdi Bilal, Ebiana Victoria, Lin Jianxin, Mok Tony S K
Division of Medical Oncology, Mayo Clinic, Rochester, Minnesota.
Yale Comprehensive Cancer Center, Yale University School of Medicine, New Haven, Connecticut.
JTO Clin Res Rep. 2021 Jul 1;2(8):100205. doi: 10.1016/j.jtocrr.2021.100205. eCollection 2021 Aug.
We retrospectively evaluated outcomes in patients with programmed death-ligand 1 (PD-L1)-positive non-small-cell lung cancer (NSCLC) to determine whether baseline (i.e., at study enrollment) brain metastases were associated with the efficacy of pembrolizumab versus chemotherapy.
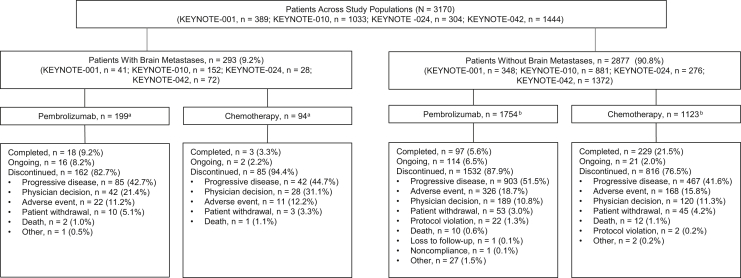
We pooled data for patients with previously treated or untreated PD-L1‒positive (tumor proportion score [TPS], ≥1%) advanced or metastatic NSCLC in KEYNOTE-001 (NCT01295827), KEYNOTE-010 (NCT01905657), KEYNOTE-024 (NCT02142738), and KEYNOTE-042 (NCT02220894). Patients received pembrolizumab (2 mg/kg, 10 mg/kg, or 200 mg every 3 wk or 10 mg/kg every 2 wk); chemotherapy was a comparator in all studies except KEYNOTE-001. All studies included patients with previously treated, stable brain metastases.
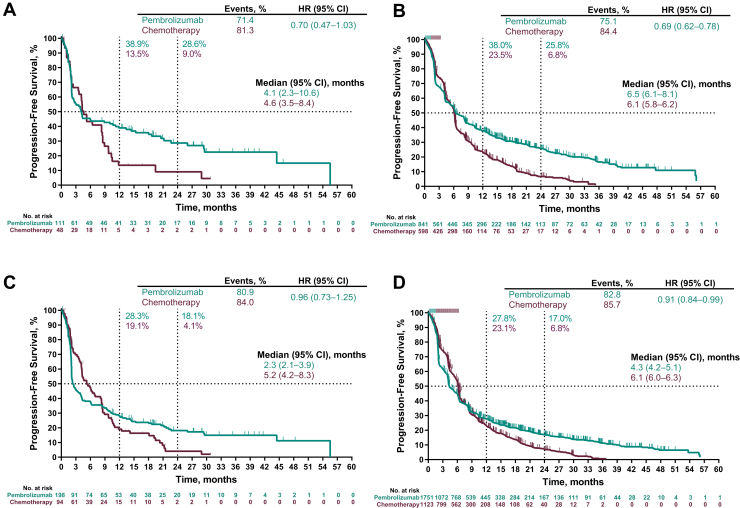
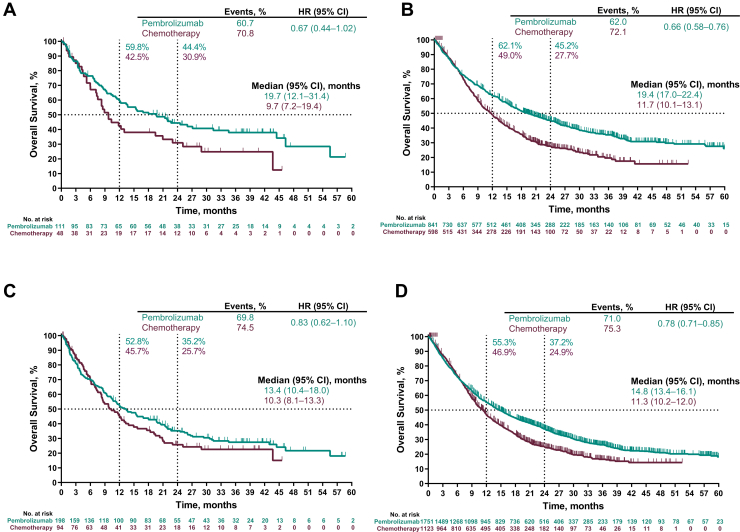
A total of 3170 patients were included, 293 (9.2%) with and 2877 (90.8%) without baseline brain metastases; median (range) follow-up at data cutoff was 12.9 (0.1‒43.7) months. Pembrolizumab improved overall survival versus chemotherapy in patients with or without baseline brain metastases: benefit was seen in patients with PD-L1 TPS ≥50% (0.67 [95% confidence intervals (CI): 0.44‒1.02] and 0.66 [95% CI: 0.58‒0.76], respectively) and PD-L1 TPS ≥1% (0.83 [95% CI: 0.62‒1.10] and 0.78 [95% CI: 0.71‒0.85], respectively). Progression-free survival was improved, objective response rates were higher, and duration of response was longer with pembrolizumab versus chemotherapy regardless of brain metastasis status. The incidence of treatment-related adverse events with pembrolizumab versus chemotherapy was 66.3% versus 84.4% in patients with brain metastases and 67.2% versus 88.3% in those without.
Pembrolizumab monotherapy improved outcomes and was associated with fewer adverse events than chemotherapy in patients with treatment-naive and previously treated PD-L1‒positive advanced/metastatic NSCLC regardless of the presence of baseline treated, stable brain metastases.
我们回顾性评估了程序性死亡配体1(PD-L1)阳性非小细胞肺癌(NSCLC)患者的预后,以确定基线(即研究入组时)脑转移是否与帕博利珠单抗对比化疗的疗效相关。
我们汇总了KEYNOTE-001(NCT01295827)、KEYNOTE-010(NCT01905657)、KEYNOTE-024(NCT02142738)和KEYNOTE-042(NCT02220894)中既往接受过治疗或未接受过治疗的PD-L1阳性(肿瘤比例评分 [TPS],≥1%)晚期或转移性NSCLC患者的数据。患者接受帕博利珠单抗(2 mg/kg、10 mg/kg,每3周一次或200 mg,或每2周一次10 mg/kg);除KEYNOTE-001外,所有研究中化疗均作为对照。所有研究均纳入了既往接受过治疗且脑转移稳定的患者。
共纳入3170例患者,293例(9.2%)有基线脑转移,2877例(90.8%)无基线脑转移;数据截止时的中位(范围)随访时间为12.9(0.1‒43.7)个月。无论有无基线脑转移,帕博利珠单抗对比化疗均改善了总生存期:PD-L1 TPS≥50%的患者(分别为0.67 [95%置信区间(CI):0.44‒1.02]和0.66 [95% CI:0.58‒0.76])以及PD-L1 TPS≥1%的患者(分别为0.83 [95% CI:0.62‒1.10]和0.78 [95% CI:0.71‒0.85])均观察到获益。无论脑转移状态如何,帕博利珠单抗对比化疗均改善了无进展生存期,提高了客观缓解率,延长了缓解持续时间。有脑转移的患者中,帕博利珠单抗与化疗相关的治疗不良事件发生率分别为66.3%和84.4%,无脑转移的患者中分别为67.2%和88.3%。
无论有无基线接受过治疗且稳定的脑转移,帕博利珠单抗单药治疗均改善了初治及既往接受过治疗的PD-L1阳性晚期/转移性NSCLC患者的预后,且不良事件少于化疗。