Gerhardt Kristin, Jentzsch Madlen, Georgi Thomas, Sretenović Aleksandra, Cross Michael, Bach Enrica, Monecke Astrid, Leiblein Sabine, Hoffmann Sandra, Todorović Milena, Bila Jelena, Sabri Osama, Schwind Sebastian, Franke Georg-Nikolaus, Platzbecker Uwe, Vučinić Vladan
Leipzig Medical Center, Clinic and Policlinic for Hematology and Cell Therapy, University of Leipzig, Leipzig, Germany.
Leipzig Medical Center, Department of Nuclear Medicine, University of Leipzig, Leipzig, Germany.
Front Oncol. 2021 Sep 16;11:737645. doi: 10.3389/fonc.2021.737645. eCollection 2021.
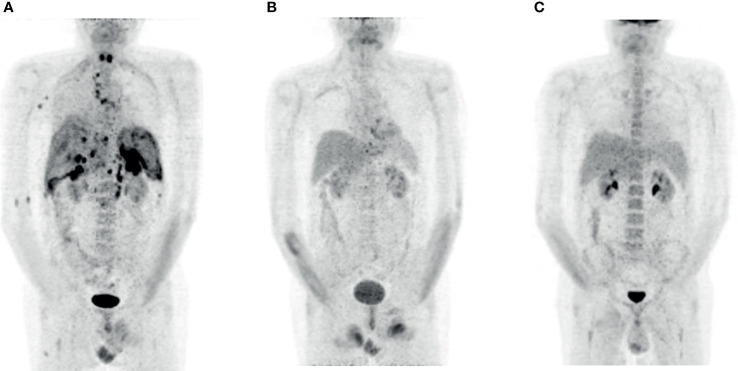
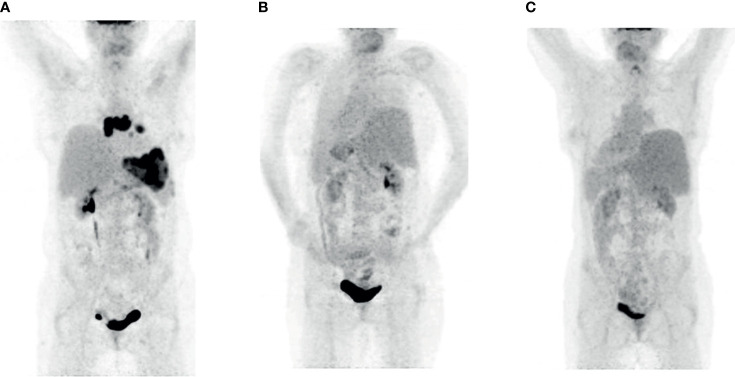
Up to 60% of patients with aggressive B-cell lymphoma who receive chimeric antigen receptor (CAR) T-cell therapy experience treatment failure and subsequently have a poor prognosis. Allogeneic hematopoietic stem cell transplantation (alloHSCT) remains a potentially curative approach for patients in this situation. Induction of a deep response prior to alloHSCT is crucial for long-term outcomes, but the optimal bridging strategy following relapse after CAR T-cell therapy has not yet been established. Polatuzumab vedotin, an antibody drug conjugate targeting CD79b, is a novel treatment option for use in combination with rituximab and bendamustine (Pola-BR) in relapsed or refractory disease. Patients: We report two heavily pretreated patients with primary refractory diffuse large B-cell lymphoma (DLBCL) and primary mediastinal B-cell lymphoma (PMBCL) respectively who relapsed after therapy with CAR T-cells with both nodal and extranodal manifestations of the disease. After application of three courses of Pola-BR both patients achieved a complete metabolic remission. Both patients underwent alloHSCT from a human leukocyte antigen (HLA)-mismatched donor following conditioning with busulfan and fludarabine and are disease free 362 days and 195 days after alloHSCT respectively. We conclude that Pola-BR can be an effective bridging therapy before alloHSCT of patients relapsing after CAR T-cell therapy. Further studies will be necessary to define the depth and durability of remission of this salvage regimen before alloHSCT.
接受嵌合抗原受体(CAR)T细胞疗法的侵袭性B细胞淋巴瘤患者中,高达60%会出现治疗失败,随后预后不良。同种异体造血干细胞移植(alloHSCT)对处于这种情况的患者而言仍是一种潜在的治愈方法。在alloHSCT前诱导深度缓解对长期预后至关重要,但CAR T细胞疗法后复发的最佳桥接策略尚未确立。泊洛妥珠单抗,一种靶向CD79b的抗体药物偶联物,是一种用于复发或难治性疾病联合利妥昔单抗和苯达莫司汀(Pola-BR)的新型治疗选择。患者:我们报告了两名分别患有原发性难治性弥漫性大B细胞淋巴瘤(DLBCL)和原发性纵隔B细胞淋巴瘤(PMBCL)且经过大量预处理的患者,他们在接受CAR T细胞治疗后复发,疾病有淋巴结和结外表现。应用三个疗程的Pola-BR后,两名患者均实现了完全代谢缓解。两名患者在接受白消安和氟达拉滨预处理后,均接受了来自人类白细胞抗原(HLA)配型不合供体的alloHSCT,分别在alloHSCT后362天和195天无病生存。我们得出结论,Pola-BR可以作为CAR T细胞治疗后复发患者alloHSCT前的有效桥接疗法。有必要进行进一步研究以明确这种挽救方案在alloHSCT前缓解的深度和持久性。