Teunissen Frederik R, Wortel Ruud C, Hes Jochem, Willigenburg Thomas, de Groot-van Breugel Eline N, de Boer Johannes C J, van Melick Harm H E, Verkooijen Helena M, van der Voort van Zyp Jochem R N
Department of Radiation Oncology, University Medical Center Utrecht, Utrecht, The Netherlands.
Department of Urology, University Medical Center Utrecht, Utrecht, The Netherlands.
Phys Imaging Radiat Oncol. 2021 Sep 21;20:5-10. doi: 10.1016/j.phro.2021.09.002. eCollection 2021 Oct.
Erectile dysfunction is a common adverse effect of external beam radiation therapy for localized prostate cancer (PCa), likely as a result of damage to neural and vascular tissue. Magnetic resonance-guided online adaptive radiotherapy (MRgRT) enables high-resolution MR imaging and paves the way for neurovascular-sparing approaches, potentially lowering erectile dysfunction after radiotherapy for PCa. The aim of this study was to assess the planning feasibility of neurovascular-sparing MRgRT for localized PCa.
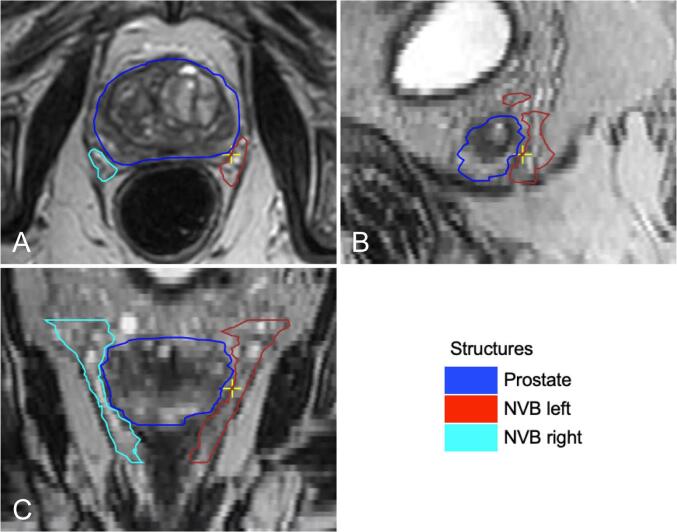
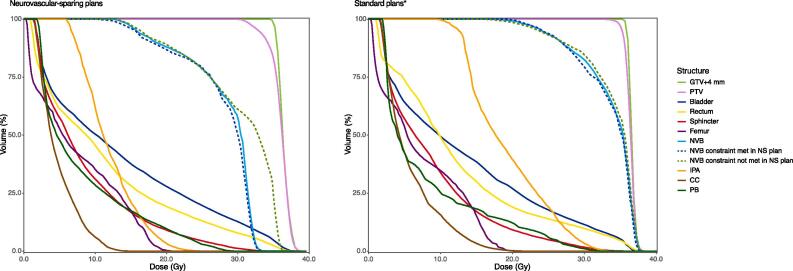
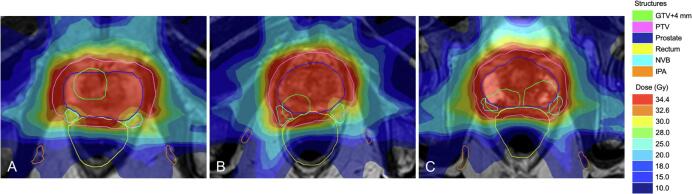
Twenty consecutive localized PCa patients, treated with standard 5×7.25 Gy MRgRT, were included. For these patients, neurovascular-sparing 5×7.25 Gy MRgRT plans were generated Dose constraints for the neurovascular bundle (NVB), the internal pudendal artery (IPA), the corpus cavernosum (CC), and the penile bulb (PB) were established. Doses to regions of interest were compared between the neurovascular-sparing plans and the standard clinical pre-treatment plans.
Neurovascular-sparing constraints for the CC, and PB were met in all 20 patients. For the IPA, constraints were met in 19 (95%) patients bilaterally and 1 (5%) patient unilaterally. Constraints for the NVB were met in 8 (40%) patients bilaterally, in 8 (40%) patients unilaterally, and were not met in 4 (20%) patients. NVB constraints were not met when gross tumor volume (GTV) was located dorsolaterally in the prostate. Dose to the NVB, IPA, and CC was significantly lower in the neurovascular-sparing plans.
Neurovascular-sparing MRgRT for localized PCa is feasible in the planning setting. The extent of NVB sparing largely depends on the patient's GTV location in relation to the NVB.
勃起功能障碍是局限性前列腺癌(PCa)外照射放疗的常见不良反应,可能是神经和血管组织受损所致。磁共振引导的在线自适应放疗(MRgRT)可实现高分辨率磁共振成像,为保留神经血管的方法铺平了道路,有可能降低PCa放疗后的勃起功能障碍。本研究的目的是评估保留神经血管的MRgRT用于局限性PCa的计划可行性。
纳入连续20例接受标准5×7.25 Gy MRgRT治疗的局限性PCa患者。为这些患者制定了保留神经血管的5×7.25 Gy MRgRT计划。确定了神经血管束(NVB)、阴部内动脉(IPA)、海绵体(CC)和阴茎球部(PB)的剂量限制。比较了保留神经血管的计划与标准临床治疗前计划中感兴趣区域的剂量。
所有20例患者的CC和PB均满足保留神经血管的限制。对于IPA,19例(95%)患者双侧满足限制,1例(5%)患者单侧满足限制。NVB的限制在8例(40%)患者双侧、8例(40%)患者单侧得到满足,4例(20%)患者未得到满足。当大体肿瘤体积(GTV)位于前列腺背外侧时,NVB限制未得到满足。保留神经血管的计划中NVB、IPA和CC的剂量显著降低。
在计划制定中,保留神经血管的MRgRT用于局限性PCa是可行的。NVB保留的程度很大程度上取决于患者GTV相对于NVB的位置。