Brand Victor J, Rossi Linda, Milder Maaike T W, Froklage Femke E, Tree Alison C, Hoogeman Mischa S, Incrocci Luca
Erasmus MC Cancer Institute, University Medical Centre Rotterdam, Department of Radiotherapy, UK.
The Royal Marsden Hospital, London, UK.
Clin Transl Radiat Oncol. 2025 Apr 9;53:100959. doi: 10.1016/j.ctro.2025.100959. eCollection 2025 Jul.
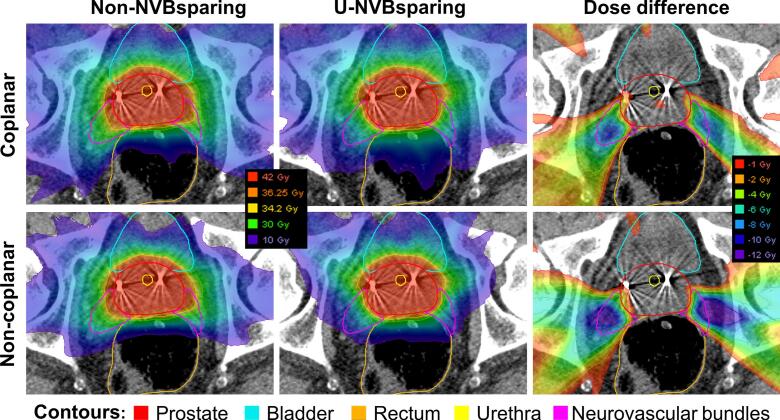
Radiation damage to the neurovascular bundles (NVB) has been linked to erectile dysfunction after prostate cancer radiotherapy (PCa). NVB sparing using coplanar and non-coplanar automated treatment planning is presented here in two settings: (1) without compromising target coverage, (2) allowing target coverage compromise.
20 previously treated patients with localized PCa. Based on a MRI-CT match, the NVB were retrospectively delineated. All treatment plans (5 × 7.25 Gy) were automatically generated using Erasmus-iCycle (in-house automated treatment planning algorithm). Non-NVB sparing (non-NVBsparing) plans and NVB sparing plans in two settings were generated: (1) uncompromised NVB sparing (u-NVBsparing; maintaining target coverage) (2) and compromised NVB sparing (c-NVBsparing; allowing target underdosage). Coplanar and non-coplanar beam arrangements were compared. U-NVBsparing was compared to non-NVBsparing. C-NVBsparing plans were visualized in Pareto fronts. Statistical significance (p-value < 0.05) was determined by Wilcoxon signed-rank test.
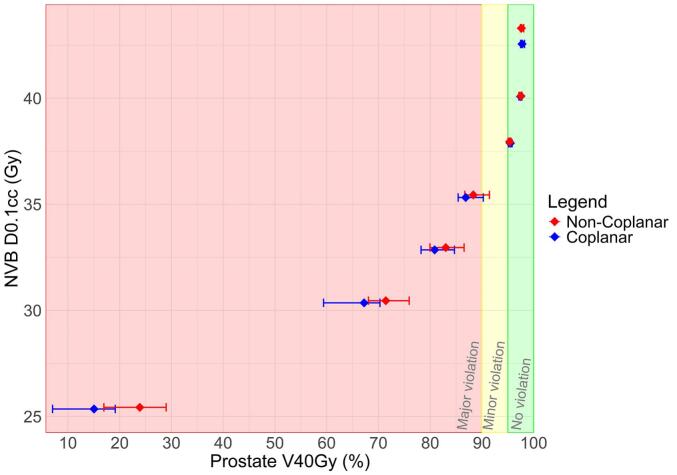
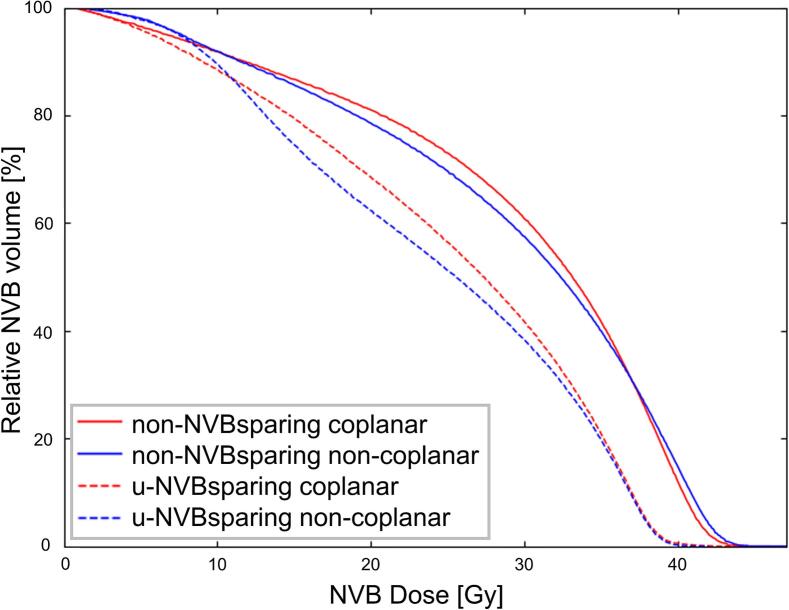
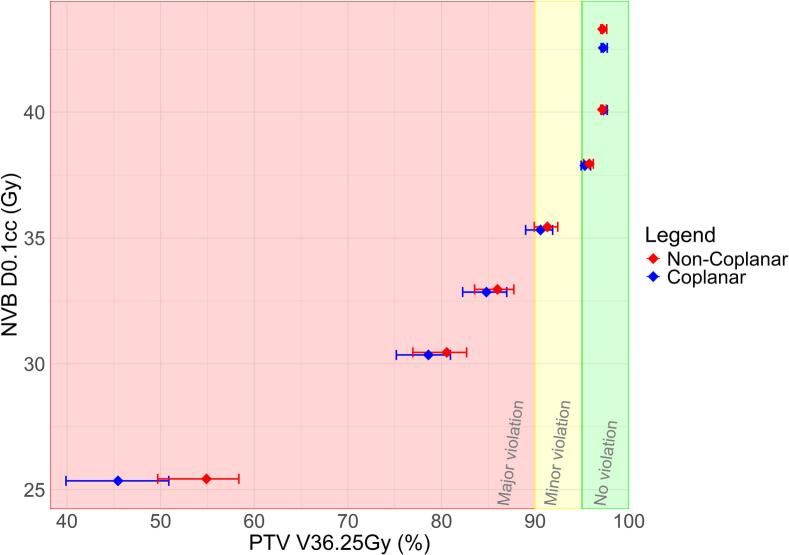
u-NVBsparing compared to non-NVBsparing plans showed statistically significant median reductions in NVB D0.1 cc (38.9 vs 42.6 Gy for coplanar; 38.9 vs 43.3 Gy for non-coplanar) and Dmean (25.6 vs 30.0 Gy for coplanar; 24.7 vs 30.2 Gy for noncoplanar). Further lowering NVB D0.1 cc in c-NVBsparing plans clearly correlated to lower target coverage. Non-coplanar c-NVBsparing plans maintained significantly higher target coverages for similar NVB D0.1 cc values, compared to coplanar plans.
NVB sparing without compromising target coverage is feasible. No clinically relevant benefit was found for non-coplanar compared to coplanar NVB sparing plans, although overall statistically superior. Further sparing of the NVB comes at the cost of target coverage, for which a Pareto front could be used as a tool in clinical practise.
前列腺癌放疗(PCa)后神经血管束(NVB)的放射性损伤与勃起功能障碍有关。本文介绍了在两种情况下使用共面和非共面自动治疗计划来保留NVB:(1)不影响靶区覆盖,(2)允许靶区覆盖妥协。
20例既往接受过治疗的局限性PCa患者。基于MRI-CT匹配,对NVB进行回顾性勾画。所有治疗计划(5×7.25 Gy)均使用伊拉斯谟-iCycle(内部自动治疗计划算法)自动生成。生成了非NVB保留(非NVBsparing)计划和两种情况下的NVB保留计划:(1)无妥协的NVB保留(u-NVBsparing;维持靶区覆盖)(2)和妥协的NVB保留(c-NVBsparing;允许靶区剂量不足)。比较了共面和非共面射束排列。将u-NVBsparing与非NVBsparing进行比较。c-NVBsparing计划在帕累托前沿进行可视化。通过Wilcoxon符号秩检验确定统计学显著性(p值<0.05)。
与非NVBsparing计划相比,u-NVBsparing显示NVB D0.1 cc(共面时为38.9 vs 42.6 Gy;非共面时为38.9 vs 43.3 Gy)和Dmean(共面时为25.6 vs 30.0 Gy;非共面时为24.7 vs 30.2 Gy)的中位数有统计学显著降低。在c-NVBsparing计划中进一步降低NVB D0.1 cc与较低的靶区覆盖明显相关。与共面计划相比,非共面c-NVBsparing计划在相似的NVB D0.1 cc值下维持了显著更高的靶区覆盖。
在不影响靶区覆盖的情况下保留NVB是可行的。与共面NVB保留计划相比,非共面计划虽总体在统计学上更优,但未发现临床相关益处。进一步保留NVB是以靶区覆盖为代价的,为此帕累托前沿可作为临床实践中的一种工具。