Appelt K, Takes M, Zech C J, Blackham K A, Schubert T
Radiology and Nuclear Medicine Clinic, University Hospital Basel, Basel, Switzerland.
Department of Neuroradiology, University Hospital Zurich, Zürich, Switzerland.
CVIR Endovasc. 2021 Oct 11;4(1):74. doi: 10.1186/s42155-021-00262-2.
The current literature on the use of brachial artery access is controversial. Some studies found increased puncture site complications. Others found no higher complication rates than in patients with femoral or radial access. The purpose of this study was to determine the impact of ultrasound (US)-guidance on access site complications.
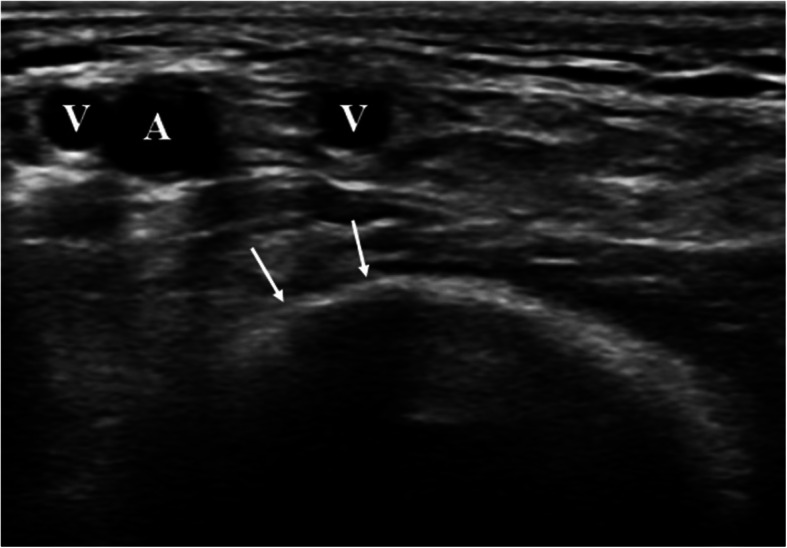
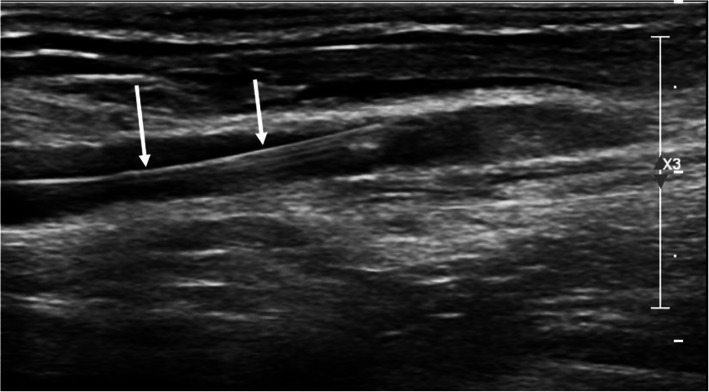
This is a single-center retrospective study of all consecutive patients with brachial arterial access for interventional procedures. Complications were classified into minor complications (conservative treatment only) and major complications (requiring surgical intervention). The brachial artery was cannulated in the antecubital fossa under US-guidance. After the intervention, manual compression or closure devices, both followed by a compression bandage for 3 h, either achieved hemostasis.
Seventy-five procedures in seventy-one patients were performed in the study period using brachial access. Access was successful in all cases (100%). Procedures in different vascular territories were performed: neurovascular (10/13.5%), upper extremity (32/43.2%), visceral (20/27.0%), and lower extremity (12/16.3%). Sheath size ranged from 3.2F to 8F (mean: 5F). Closure devices were used in 17 cases (22.7%). In total, six complications were observed (8.0%), four minor complications (5.3%, mostly puncture site hematomas), and two major complications, that needed surgical treatment (2.7%). No brachial artery thrombosis or upper extremity ischemia occurred.
Exclusive use of US-guidance resulted in a low risk of brachial artery access site complications in our study compared to the literature. US-guidance has been proven to reduce the risk of access site complications in several studies in femoral access. In addition, brachial artery access yields a high technical success rate and requires no additional injection of spasmolytic medication. Sheath size was the single significant predictor for complications.
目前关于使用肱动脉入路的文献存在争议。一些研究发现穿刺部位并发症增加。另一些研究则发现其并发症发生率并不高于股动脉或桡动脉入路的患者。本研究的目的是确定超声(US)引导对入路部位并发症的影响。
这是一项对所有连续接受肱动脉入路进行介入手术的患者的单中心回顾性研究。并发症分为轻微并发症(仅需保守治疗)和严重并发症(需要手术干预)。在超声引导下于肘前窝穿刺肱动脉。介入操作后,采用手动压迫或闭合装置,之后均用压迫绷带压迫3小时以实现止血。
在研究期间,对71例患者进行了75例使用肱动脉入路的手术。所有病例入路均成功(100%)。进行了不同血管区域的手术:神经血管(10/13.5%)、上肢(32/43.2%)、内脏(20/27.0%)和下肢(12/16.3%)。鞘管尺寸范围为3.2F至8F(平均:5F)。17例(22.7%)使用了闭合装置。总共观察到6例并发症(8.0%),4例轻微并发症(5.3%,主要为穿刺部位血肿),2例严重并发症需要手术治疗(2.7%)。未发生肱动脉血栓形成或上肢缺血。
与文献报道相比,在我们的研究中单纯使用超声引导导致肱动脉入路部位并发症风险较低。在多项股动脉入路研究中已证明超声引导可降低入路部位并发症的风险。此外,肱动脉入路技术成功率高,且无需额外注射解痉药物。鞘管尺寸是并发症的唯一显著预测因素。