Sharett Institute of Oncology, Hadassah-Hebrew University Medical Center, Jerusalem, Israel; Faculty of Medicine, The Hebrew University, Jerusalem, Israel.
Faculty of Medicine, The Hebrew University, Jerusalem, Israel; Department of Nephrology and Hypertension, Hadassah-Hebrew University Medical Center, Jerusalem, Israel.
ESMO Open. 2021 Dec;6(6):100283. doi: 10.1016/j.esmoop.2021.100283. Epub 2021 Sep 27.
It was shown that immunocompromised patients have significantly reduced immunologic responses to COVID-19 vaccines. The immunogenicity of COVID-19 vaccine/infection in patients with solid tumors is reduced. We evaluated the immunologic response to COVID-19 and/or the BNT162b2 mRNA COVID-19 vaccine among cancer patients on active treatments and reviewed previous literature to identify subgroups that may require third vaccination.
Anti-SARS-CoV-2 S1/S2 antibodies were measured in a cohort of 202 cancer patients on active treatment with chemotherapy (96), immunologic (52), biologic (46), and hormonal (12) treatments for early (n = 66, 32.7%) or metastatic disease (n = 136, 67.3%). Of those, 172 had received two vaccine doses, and 30 had COVID-19 infection (20/30 also received one dose of vaccine). Specific anti-S receptor-binding domain antibodies were further measured in patients with equivocal anti-S1/S2 results.
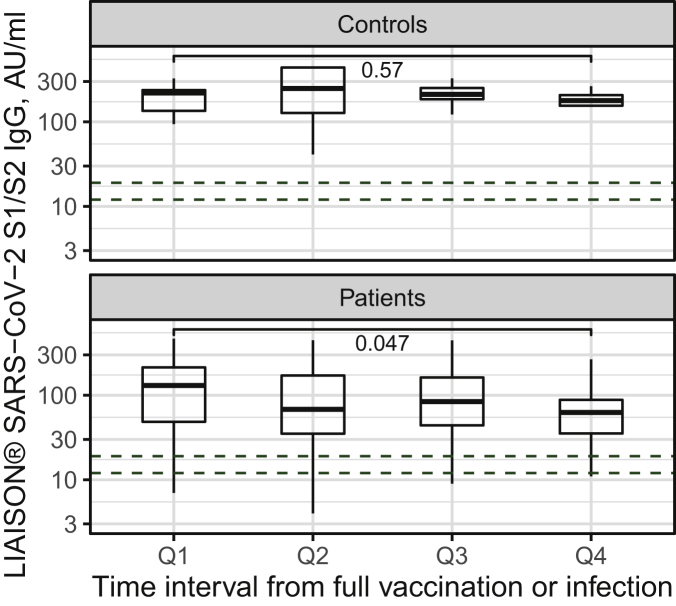
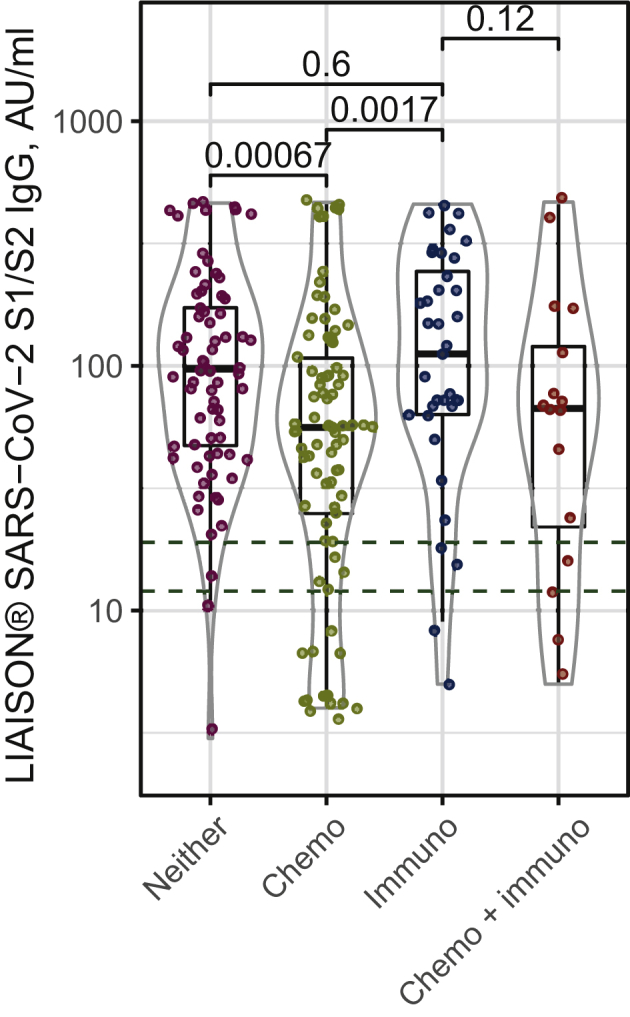
Among cancer patients, the SARS-CoV-2 antibody response rate was 89.1% (180/202) after COVID-19 vaccination or infection and 87.2% (150/172) in patients after vaccination without a history of COVID-19, compared with 100% positive serologic tests in a control group of 30 health care workers (P < 0.001). Chemotherapy treatment was independently associated with significantly reduced humoral response to infection or vaccination, with an 81.3% response rate, compared with 96.2% in patients on other treatments (P = 0.001). In vaccinated patients on chemotherapy, the positive response rate was 77.5%. In a multiple regression model, a neutralizing antibody titer (>60 AU/ml) was more likely with immunotherapy (odds ratio 2.44) and less likely with chemotherapy (odds ratio 0.39).
Overall, both COVID-19 vaccine and natural infection are highly immunogenic among cancer patients. Our study, however, identifies those under chemotherapy as significantly less responsive, and with lower antibody levels. These findings justify close virological and serological surveillance along with consideration of these patients for booster (third dose) vaccine prioritization, as new highly spreading SARS-CoV-2 variants emerge.
免疫功能低下的患者对 COVID-19 疫苗的免疫反应明显降低。患有实体瘤的 COVID-19 疫苗/感染的免疫原性降低。我们评估了癌症患者对 COVID-19 的免疫反应和/或 BNT162b2 mRNA COVID-19 疫苗的免疫反应,并回顾了先前的文献,以确定可能需要第三次接种的亚组。
在一个由 202 名正在接受化疗(96 人)、免疫治疗(52 人)、生物治疗(46 人)和激素治疗(12 人)的癌症患者队列中测量了针对 SARS-CoV-2 S1/S2 的抗体。这些患者中,66 例为早期疾病(n=66,32.7%),136 例为转移性疾病(n=136,67.3%)。其中 172 人接受了两剂疫苗接种,30 人感染了 COVID-19(20/30 人还接种了一剂疫苗)。在抗体 S1/S2 结果不确定的患者中,进一步测量了针对 S 受体结合域的特异性抗体。
在癌症患者中,COVID-19 疫苗接种或感染后 SARS-CoV-2 抗体的反应率为 89.1%(180/202),而无 COVID-19 感染史的疫苗接种患者中为 87.2%(150/172),而在 30 名医护人员对照组中,血清学检测结果均为阳性(P<0.001)。化疗治疗与感染或接种疫苗后的体液反应显著降低相关,反应率为 81.3%,而其他治疗患者的反应率为 96.2%(P=0.001)。在接受化疗的接种疫苗患者中,阳性反应率为 77.5%。在多因素回归模型中,免疫治疗(优势比 2.44)更有可能产生中和抗体滴度(>60 AU/ml),而化疗(优势比 0.39)则不太可能。
总体而言,癌症患者对 COVID-19 疫苗和自然感染均具有高度的免疫原性。然而,我们的研究发现,接受化疗的患者反应明显降低,抗体水平也较低。这些发现证明了在新的高传播 SARS-CoV-2 变体出现时,需要对这些患者进行密切的病毒学和血清学监测,并考虑为这些患者接种加强(第三剂)疫苗。