Noten Anna M E, Kammeraad Janneke A E, Ramdat Misier Nawin L, Wijchers Sip, van Beynum Ingrid M, Dalinghaus Michiel, Krasemann Thomas B, Yap Sing-Chien, de Groot Natasja M S, Szili-Torok Tamas
Department of Cardiology, Erasmus MC, University Medical Center, Rotterdam, the Netherlands.
Department of Pediatric Cardiology, Sophia Children's Hospital, Erasmus MC, University Medical Center, Rotterdam, the Netherlands.
Int J Cardiol Heart Vasc. 2021 Oct 1;37:100881. doi: 10.1016/j.ijcha.2021.100881. eCollection 2021 Dec.
Catheter ablation (CA) is the first-choice treatment for tachyarrhythmia in children. Currently available CA techniques differ in mechanism of catheter navigation and energy sources. There are no large studies comparing long-term outcomes between available CA techniques in a pediatric population with atrioventricular reentry tachycardia (AVRT) or atrioventricular nodal reentry tachycardia (AVNRT) mechanisms.
This study aimed to compare procedural and long-term outcomes of remote magnetic navigation-guided radiofrequency (RF) ablation (RMN), manual-guided RF ablation (MAN) and manual-guided cryoablation (CRYO).
This single-center, retrospective study included all first consecutive CA procedures for AVRT or AVNRT performed in children without structural heart disease from 2008 to 2019. Three study groups were defined by the ablation technique used: RMN, MAN or CRYO. Primary outcome was long-term recurrence of tachyarrhythmia.
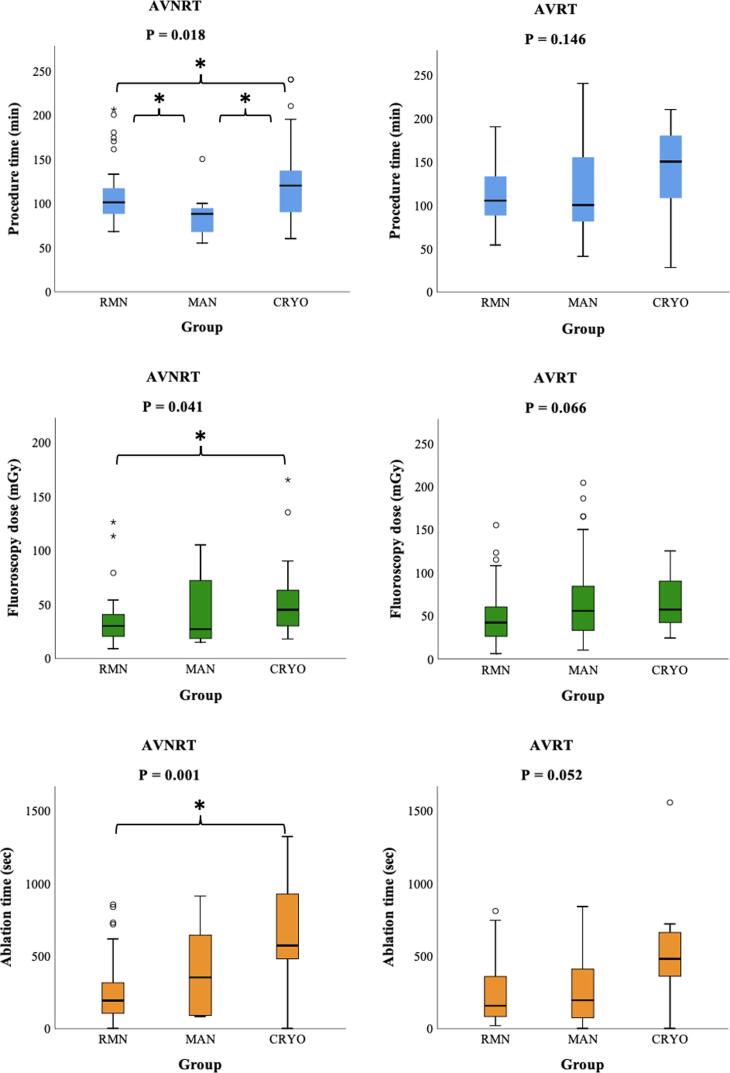
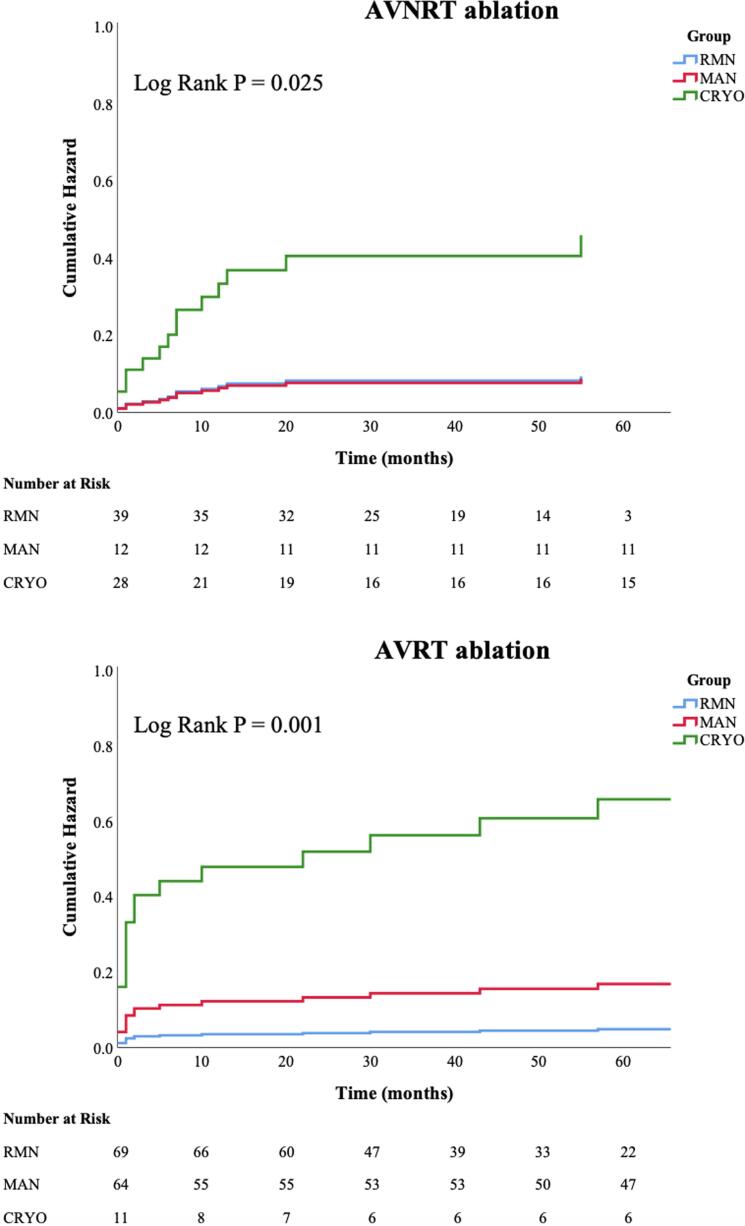
In total, we included 223 patients, aged 14 (IQR 12-16) years; weighting 56 (IQR 47-65) kilograms. In total, 108 procedures were performed using RMN, 76 using MAN and 39 using CRYO. RMN had significantly lower recurrence rates compared to MAN and CRYO at mean follow-up of 5.5 ± 2.9 years (AVRT: 4.3% versus 15.6% versus 54.5%, P < 0.001; AVNRT: 7.7% versus 8.3% versus 35.7%, P = 0.008; for RMN versus MAN versus CRYO respectively). In AVNRT ablation, RMN had significantly lower fluoroscopy doses compared to CRYO [30 (IQR 20-41) versus 45 (IQR 29-65) mGy, P = 0.040).
In pediatric patients without structural heart disease who underwent their first AV(N)RT ablation, RMN has superior long-term outcomes compared to MAN and CRYO, in addition to favorable fluoroscopy doses.
导管消融术(CA)是儿童快速性心律失常的首选治疗方法。目前可用的CA技术在导管导航机制和能量来源方面存在差异。在患有房室折返性心动过速(AVRT)或房室结折返性心动过速(AVNRT)机制的儿科人群中,尚无大型研究比较现有CA技术之间的长期疗效。
本研究旨在比较远程磁导航引导下的射频(RF)消融术(RMN)、手动引导下的RF消融术(MAN)和手动引导下的冷冻消融术(CRYO)的手术过程和长期疗效。
这项单中心回顾性研究纳入了2008年至2019年期间在无结构性心脏病的儿童中进行的所有首次连续性AVRT或AVNRT的CA手术。根据所使用的消融技术定义了三个研究组:RMN、MAN或CRYO。主要结局是快速性心律失常的长期复发。
我们总共纳入了223例患者,年龄为14(四分位间距12 - 16)岁,体重为56(四分位间距47 - 65)千克。总共进行了108例RMN手术、76例MAN手术和39例CRYO手术。在平均5.5±2.9年的随访中,RMN的复发率明显低于MAN和CRYO(AVRT:4.3%对15.6%对54.5%,P<0.001;AVNRT:7.7%对8.3%对35.7%,P = 0.008;分别为RMN对MAN对CRYO)。在AVNRT消融中,RMN的透视剂量明显低于CRYO [30(四分位间距20 - 41)对45(四分位间距29 - 65)mGy,P = 0.040]。
在接受首次AV(N)RT消融的无结构性心脏病的儿科患者中,RMN与MAN和CRYO相比具有更好的长期疗效,且透视剂量也更有利。