Bell Daniel, Hale Julia, Go Cara, Challis Ben G, Das Tilak, Fish Brian, Casey Ruth T
Department of Pharmacy, Cambridge University Hospital NHS Foundation Trust, Cambridge, UK.
Department of Endocrinology, Cambridge University Hospital NHS Foundation Trust, Cambridge, UK.
Endocr Connect. 2021 Nov 5;10(11):1435-1444. doi: 10.1530/EC-21-0258.
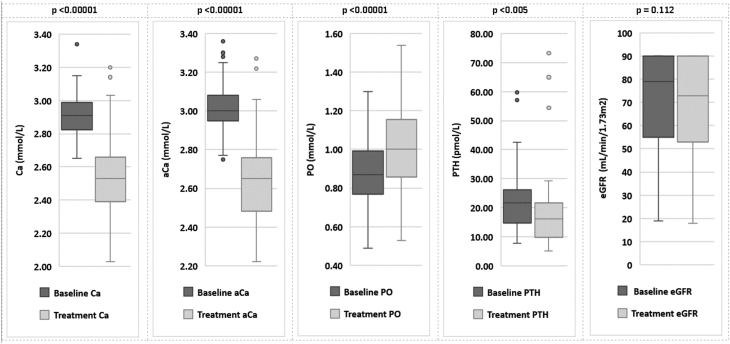
Primary hyperparathyroidism (pHPT) is a common endocrine disorder that can be cured by parathyroidectomy; patients unsuitable for surgery can be treated with cinacalcet. Availability of surgery may be reduced during COVID-19, and cinacalcet can be used as bridging therapy. In this single-centre retrospective analysis, we investigated the utility and safety of cinacalcet in patients with pHPT receiving cinacalcet between March 2019 and July 2020, including pre-parathyroidectomy bridging. We reviewed and summarised the published literature. Cinacalcet dosages were adjusted by endocrinologists to achieve target calcium < 2.70 mmol/L. Eighty-six patients were identified, with the most achieving target calcium (79.1%) with a mean dose of 39.4 mg/day (±17.1 mg/day) for a median duration of 35 weeks (1-178 weeks). Calcium was normalised in a median time of 5 weeks. The majority of patients commenced cinacalcet of 30 mg/day (78 patients) with the remainder at 60 mg/day (8 patients). Forty-seven patients commencing lower dose cinacalcet (30 mg/day) achieved target calcium without requiring 60 mg/day. Baseline PTH was significantly higher in patients requiring higher doses of cinacalcet. 18.6% of patients reported adverse reactions and 4.7% discontinued cinacalcet. Patients treated with cinacalcet pre-parathyroidectomy required a higher dose and fewer achieved target calcium compared to medical treatment with cinacalcet alone. Post-operative calcium was similar to patients who were not given pre-parathyroidectomy cinacalcet. In summary, cinacalcet at an initial dose of 30 mg/day is safe and useful for achieving target calcium in patients with symptomatic or severe hypercalcaemia in pHPT, including those treated for pre-parathyroidectomy. We propose a PTH threshold of >30 pmol/L to initiate at a higher dose of 60 mg/day.
原发性甲状旁腺功能亢进症(pHPT)是一种常见的内分泌疾病,可通过甲状旁腺切除术治愈;不适合手术的患者可用西那卡塞治疗。在新型冠状病毒肺炎疫情期间,手术的可及性可能会降低,西那卡塞可作为过渡治疗。在这项单中心回顾性分析中,我们调查了2019年3月至2020年7月期间接受西那卡塞治疗的pHPT患者使用西那卡塞的效用和安全性,包括甲状旁腺切除术前的过渡治疗。我们回顾并总结了已发表的文献。内分泌科医生调整西那卡塞剂量以实现血钙目标<2.70 mmol/L。共纳入86例患者,大多数患者(79.1%)实现了血钙目标,平均剂量为39.4 mg/天(±17.1 mg/天),中位疗程为35周(1 - 178周)。血钙在中位时间5周内恢复正常。大多数患者开始使用30 mg/天的西那卡塞(78例患者),其余患者使用60 mg/天(8例患者)。47例开始使用较低剂量西那卡塞(30 mg/天)的患者在未使用60 mg/天的情况下实现了血钙目标。需要更高剂量西那卡塞的患者基线甲状旁腺激素(PTH)显著更高。18.6%的患者报告了不良反应,4.7%的患者停用了西那卡塞。与仅接受西那卡塞药物治疗相比,甲状旁腺切除术前接受西那卡塞治疗的患者需要更高的剂量,且实现血钙目标的患者较少。术后血钙与未接受甲状旁腺切除术前使用西那卡塞治疗的患者相似。总之,初始剂量为30 mg/天的西那卡塞对于实现pHPT有症状或严重高钙血症患者(包括接受甲状旁腺切除术前治疗的患者)的血钙目标是安全且有用的。我们建议,当PTH阈值>30 pmol/L时,应开始使用更高剂量60 mg/天的西那卡塞。