Unit of Trauma and Surgical Critical Care, Division of General Surgery, Department of Surgery, Faculty of Medicine, Thammasat University, Pathumthani, 12120, Thailand.
Unit of Trauma and Surgical Critical Care, Division of General Surgery, Department of Surgery, Faculty of Medicine, Thammasat University, Pathumthani, 12120, Thailand.
Chin J Traumatol. 2022 Sep;25(5):249-256. doi: 10.1016/j.cjtee.2021.09.006. Epub 2021 Sep 20.
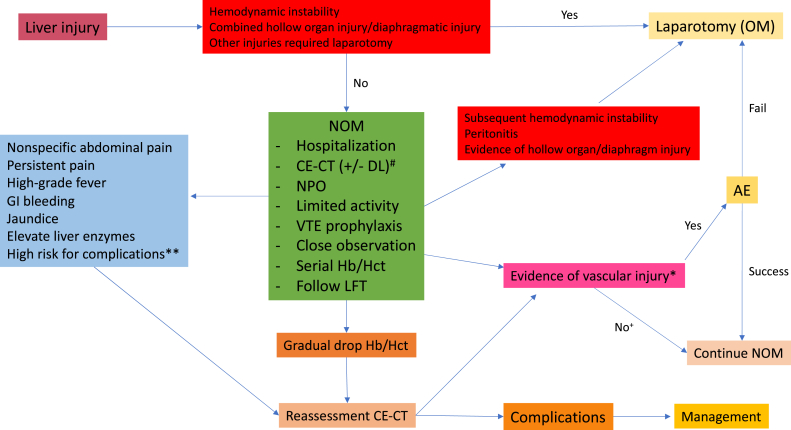
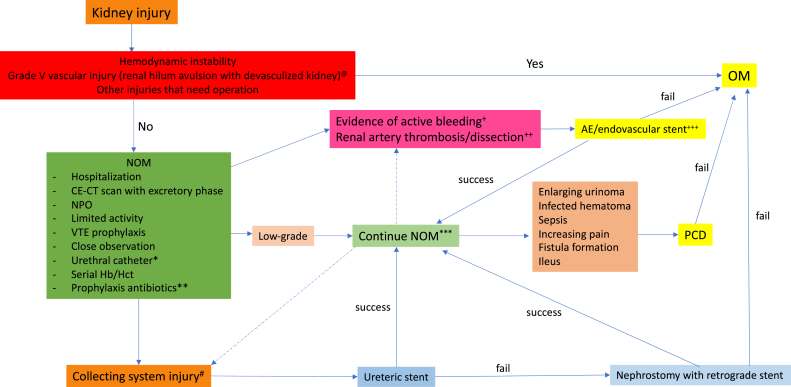
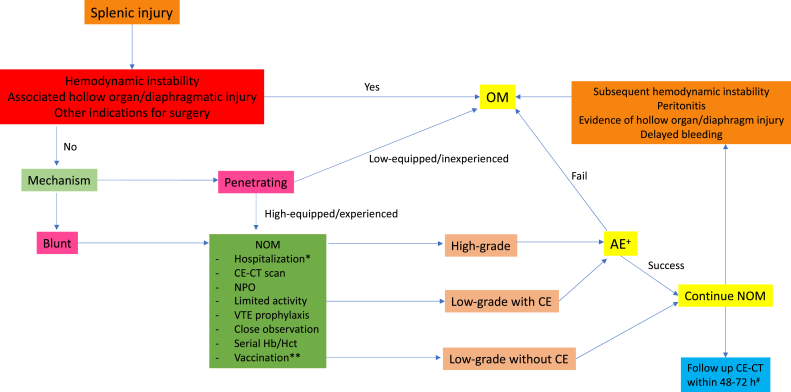
The philosophy of abdominal injury management is currently changing from mandatory exploration to selective non-operative management (NOM). The patient with hemodynamic stability and absence of peritonitis should be managed non-operatively. NOM has an overall success rate of 80%-90%. It also can reduce the rate of non-therapeutic abdominal exploration, preserve organ function, and has been defined as the safest choice in experienced centers. However, NOM carries a risk of missed injury such as hollow organ injury, diaphragm injury, and delayed hemorrhage. Adjunct therapies such as angiography with embolization, endoscopic retrograde cholangiopancreatography with stenting, and percutaneous drainage could increase the chances of successful NOM. This article aims to describe the evolution of NOM and define its place in specific abdominal solid organ injury for the practitioner who faces this problem.
腹部损伤处理的理念目前正从强制性探查转变为选择性非手术治疗(NOM)。对于血流动力学稳定且无腹膜炎的患者,应进行非手术治疗。NOM 的总体成功率为 80%-90%。它还可以降低非治疗性剖腹探查的发生率,保护器官功能,并且在有经验的中心被定义为最安全的选择。然而,NOM 存在漏诊损伤的风险,如空心器官损伤、膈肌损伤和延迟性出血。辅助治疗,如血管造影栓塞、内镜逆行胰胆管造影支架置入和经皮引流,可增加 NOM 成功的机会。本文旨在描述 NOM 的演变,并为面临这一问题的临床医生确定其在特定腹部实体器官损伤中的地位。